

Evolution of severe sleep-wake cycle disturbances following traumatic brain injury: a case study in both acute and subacute phases post-injury
- PMID: 27677675
- PMCID: PMC5039911
- DOI: 10.1186/s12883-016-0709-x
Evolution of severe sleep-wake cycle disturbances following traumatic brain injury: a case study in both acute and subacute phases post-injury
Abstract
Background: Sleep-wake disturbances are frequently reported following traumatic brain injury (TBI), but they remain poorly documented in the acute stage of injury. Little is known about their origin and evolution.
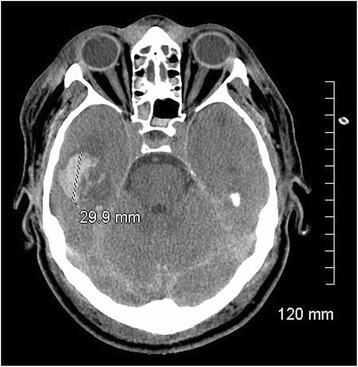
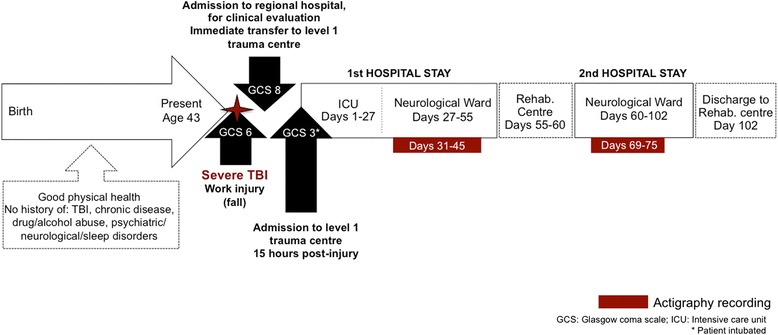
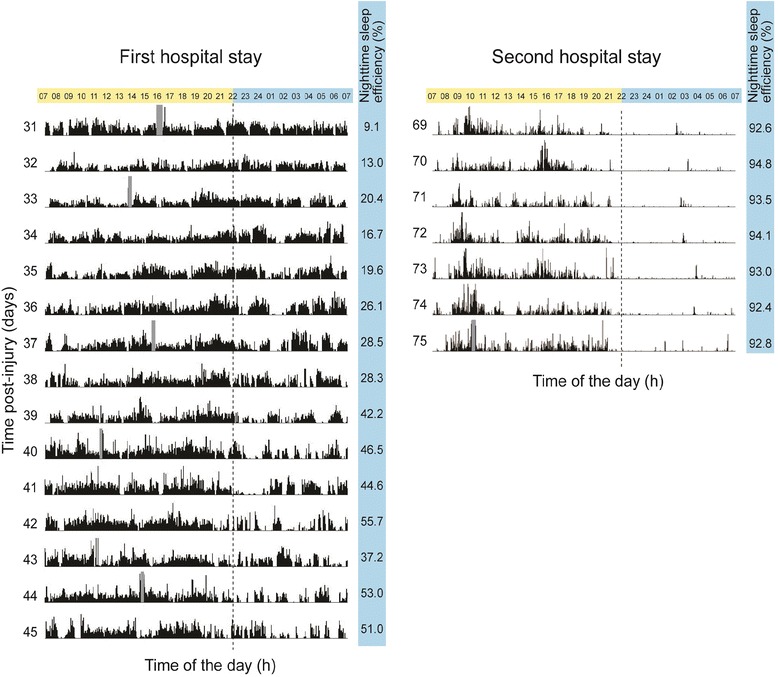
Case presentation: This study presents the case of a patient in the acute phase of a severe TBI. The patient was injured at work when falling 12 m into a mine and was hospitalized in the regular wards of a level I trauma centre. From days 31 to 45 post-injury, once he had reached a level of medical stability and continuous analgosedation had been ceased, his sleep-wake cycle was monitored using actigraphy. Results showed significant sleep-wake disturbances and severe sleep deprivation. Indeed, the patient had an average nighttime sleep efficiency of 32.7 ± 15.4 %, and only an average of 4.8 ± 1.3 h of sleep per 24-h period. After hospital discharge to the rehabilitation centre, where he remained for 5 days, the patient was readmitted to the same neurological unit for paranoid delusions. During his second hospital stay, actigraphy recordings resumed from days 69 to 75 post-injury. A major improvement in his sleep-wake cycle was observed during this second stay, with an average nighttime sleep efficiency of 96.3 ± 0.9 % and an average of 14.1 ± 0.9 h of sleep per 24-h period.
Conclusion: This study is the first to extensively document sleep-wake disturbances in both the acute and subacute phases of severe TBI. Results show that prolonged sleep deprivation can be observed after TBI, and suggest that the hospital environment only partially contributes to sleep-wake disturbances. Continuous actigraphic monitoring may prove to be a useful clinical tool in the monitoring of patients hospitalized after severe TBI in order to detect severe sleep deprivation requiring intervention. The direct impact of sleep-wake disturbances on physiological and cognitive recovery is not well understood within this population, but is worth investigating and improving.
Keywords: Actigraphy; Circadian rhythms; Neurocritical care; Neuropsychiatry; Sleep disorders; Traumatic brain injury.
Figures
References
-
- Nakase-Richardson R, Sherer M, Barnett SD, Yablon SA, Evans CC, Kretzmer T, Schwartz DJ, Modarres M. Prospective evaluation of the nature, course, and impact of acute sleep abnormality after traumatic brain injury. Arch Phys Med Rehabil. 2013;94(5):875–82. doi: 10.1016/j.apmr.2013.01.001. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
