

Patient-Centered Interventions to Improve Adherence to Statins: A Narrative Synthesis of Systematically Identified Studies
- PMID: 27677773
- PMCID: PMC5047948
- DOI: 10.1007/s40265-016-0640-x
Patient-Centered Interventions to Improve Adherence to Statins: A Narrative Synthesis of Systematically Identified Studies
Abstract
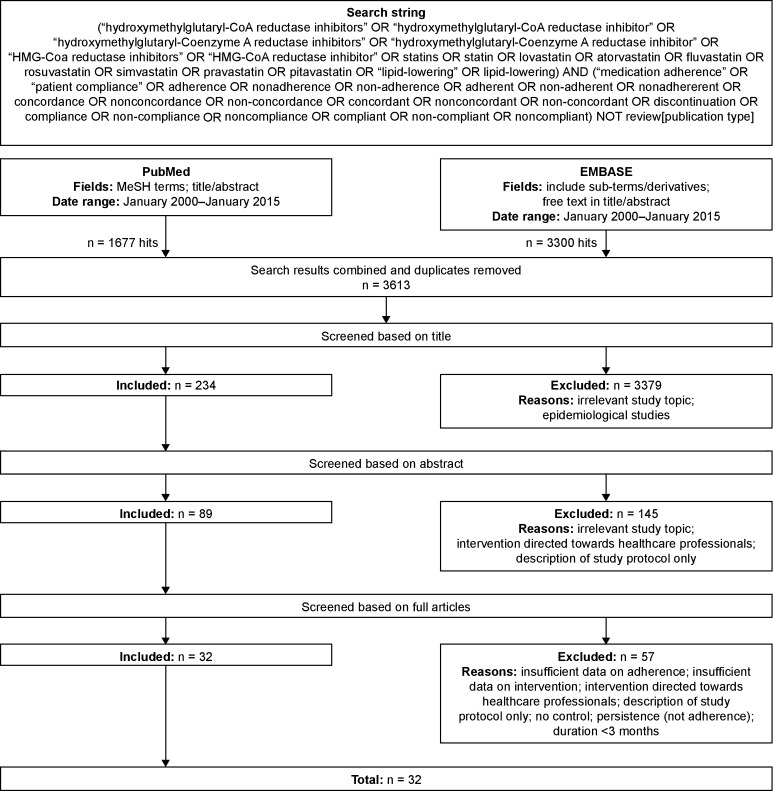
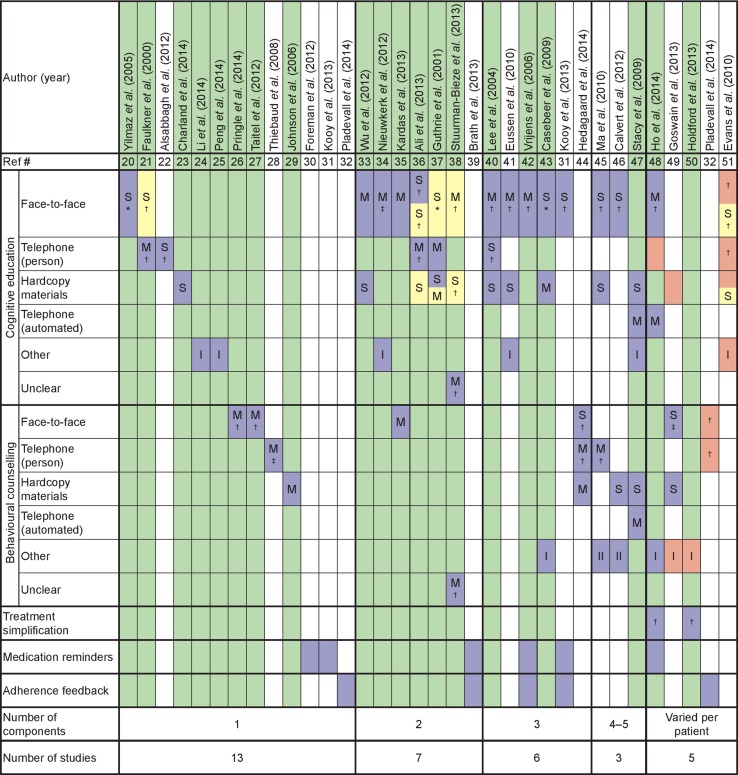
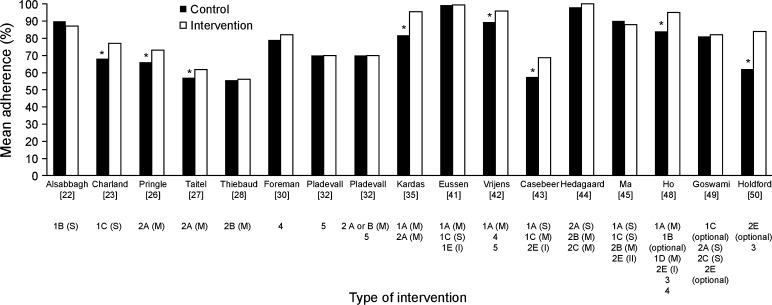
Poor adherence to statins increases cardiovascular disease risk. We systematically identified 32 controlled studies that assessed patient-centered interventions designed to improve statin adherence. The limited number of studies and variation in study characteristics precluded strict quality criteria or meta-analysis. Cognitive education or behavioural counselling delivered face-to-face multiple times consistently improved statin adherence compared with control groups (7/8 and 3/3 studies, respectively). None of four studies using medication reminders and/or adherence feedback alone reported significantly improved statin adherence. Single interventions that improved statin adherence but were not conducted face-to-face included cognitive education in the form of genetic test results (two studies) and cognitive education via a website (one study). Similar mean adherence measures were reported for 17 intervention arms and were thus compared in a sub-analysis: 8 showed significantly improved statin adherence, but effect sizes were modest (+7 to +22 % points). In three of these studies, statin adherence improved despite already being high in the control group (82-89 vs. 57-69 % in the other studies). These three studies were the only studies in this sub-analysis to include cognitive education delivered face-to-face multiple times (plus other interventions). In summary, the most consistently effective interventions for improving adherence to statins have modest effects and are resource-intensive. Research is needed to determine whether modern communications, particularly mobile health platforms (recently shown to improve medication adherence in other chronic diseases), can replicate or even enhance the successful elements of these interventions while using less time and fewer resources.
Conflict of interest statement
Compliance with Ethical StandardsFundingThis study was funded by AstraZeneca Gothenburg, Mölndal, Sweden.Conflict of interestMagnus Jörntén-Karlsson, Staffan Berg and Matti Ahlqvist are employees of AstraZeneca Gothenburg, Mölndal, Sweden, which manufactures rosuvastatin. Stéphane Pintat and Michael Molloy-Bland are employees of Oxford PharmaGenesis Ltd, which receives funding from AstraZeneca.
Figures
References
-
- World Health Organization. The World Health Report 2002. Reducing risks, promoting healthy life. 2002. http://www.who.int/whr/2002/en/. Accessed 5 May 2016.
-
- World Health Organization. Global Status Report on Noncommunicable Diseases. 2010. http://www.who.int/nmh/publications/ncd_report2010/en/. Accessed 5 May 2016.
-
- Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670–1681. doi: 10.1016/S0140-6736(10)61350-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
