

Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology
- PMID: 27677946
- PMCID: PMC5087876
- DOI: 10.1194/jlr.R071233
Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology
Abstract
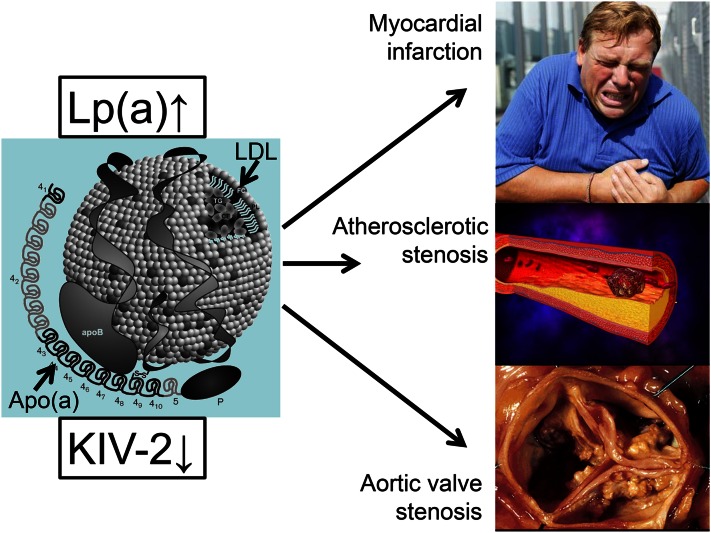
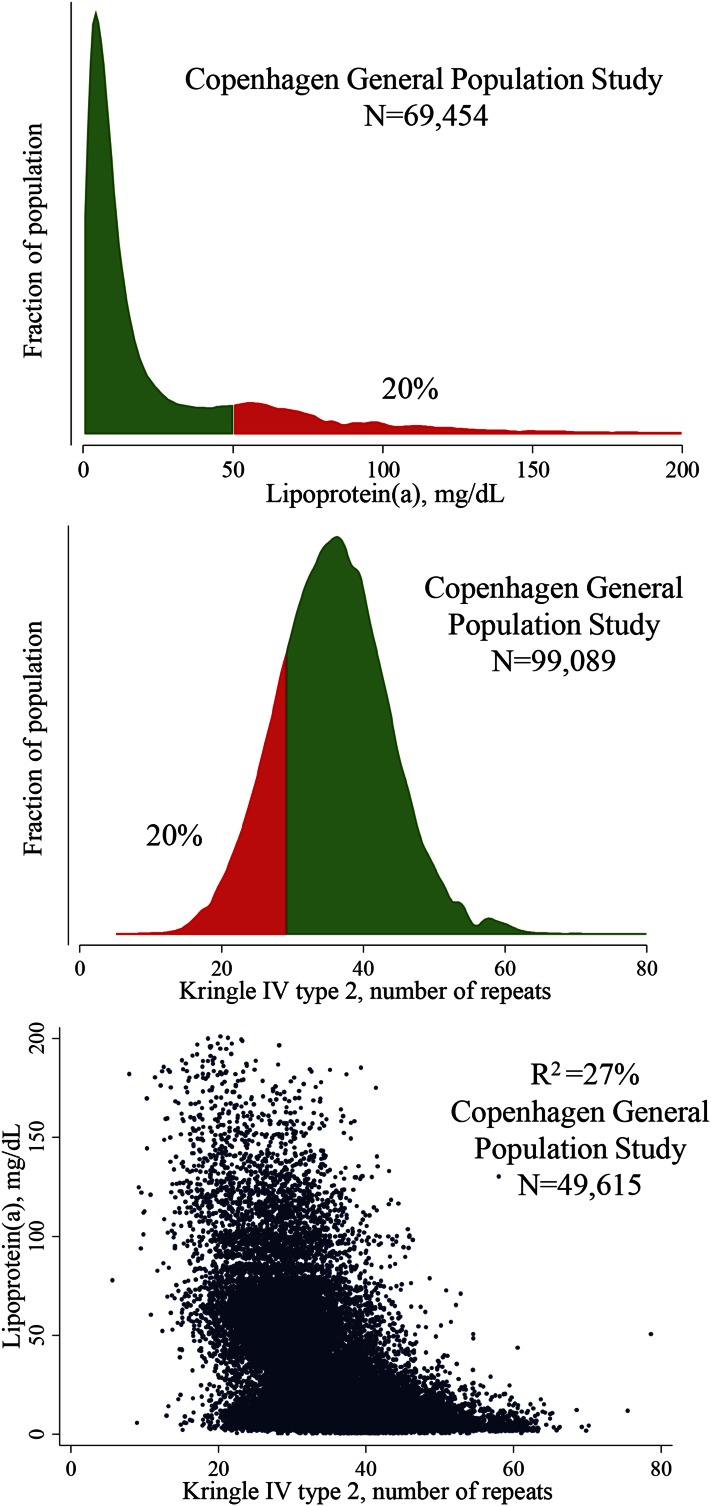
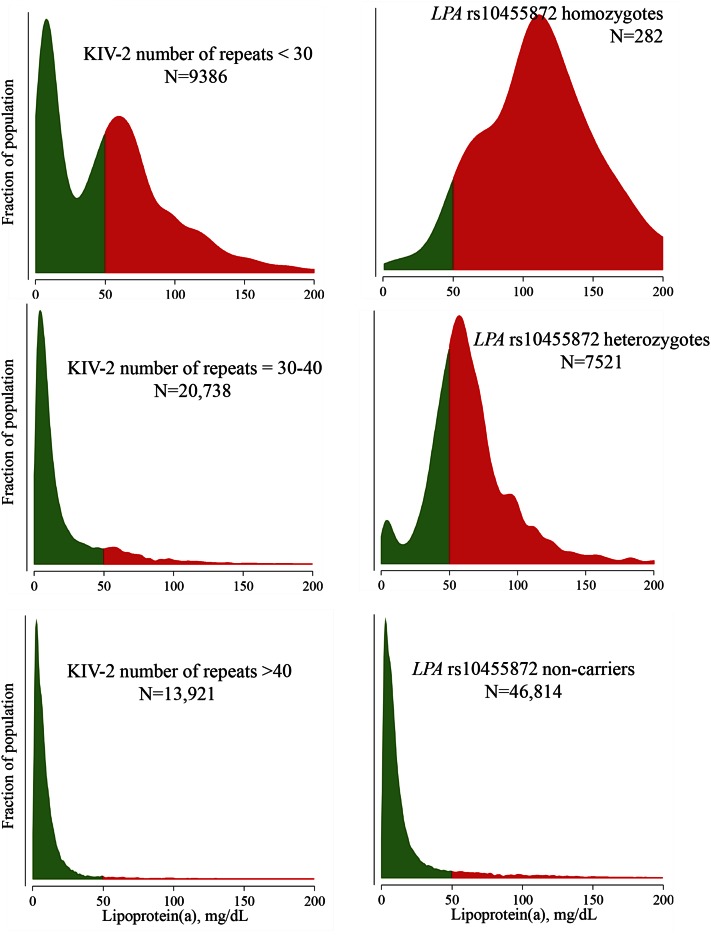
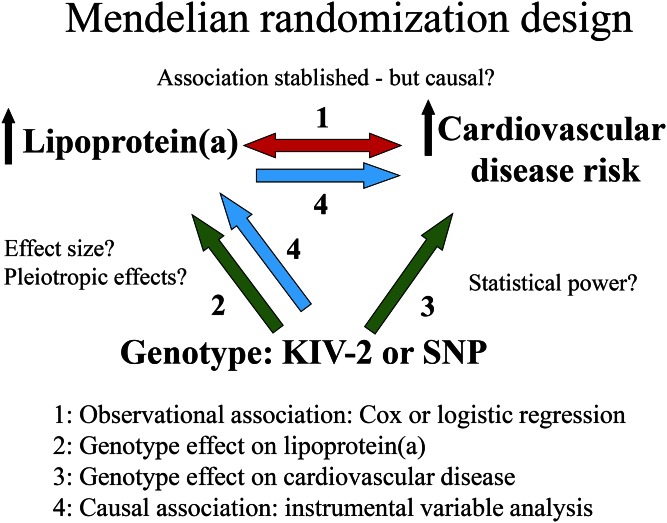
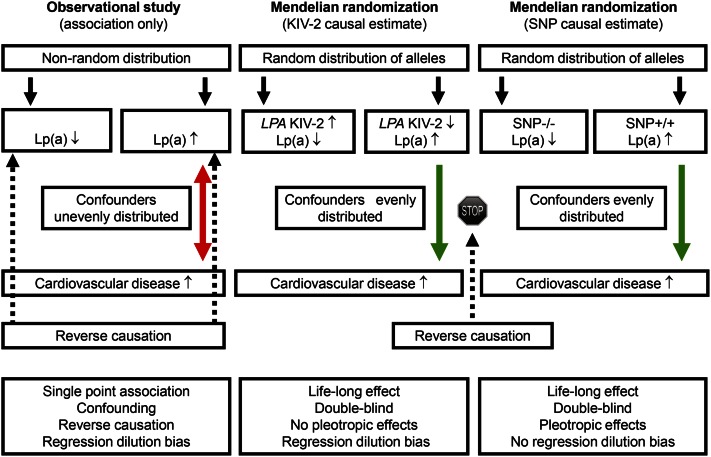
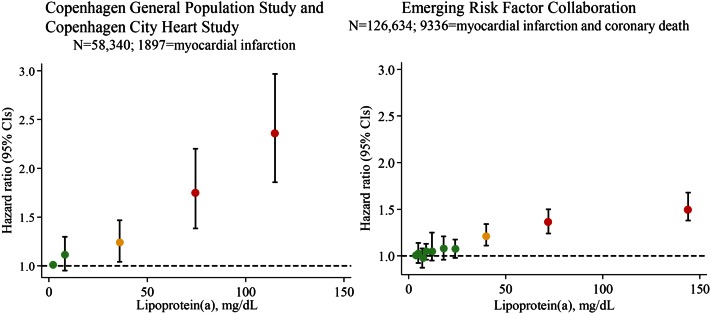
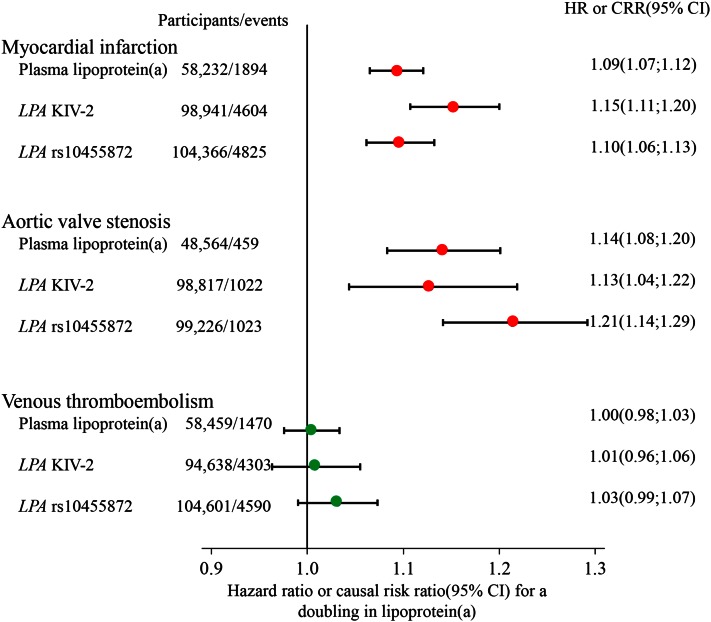
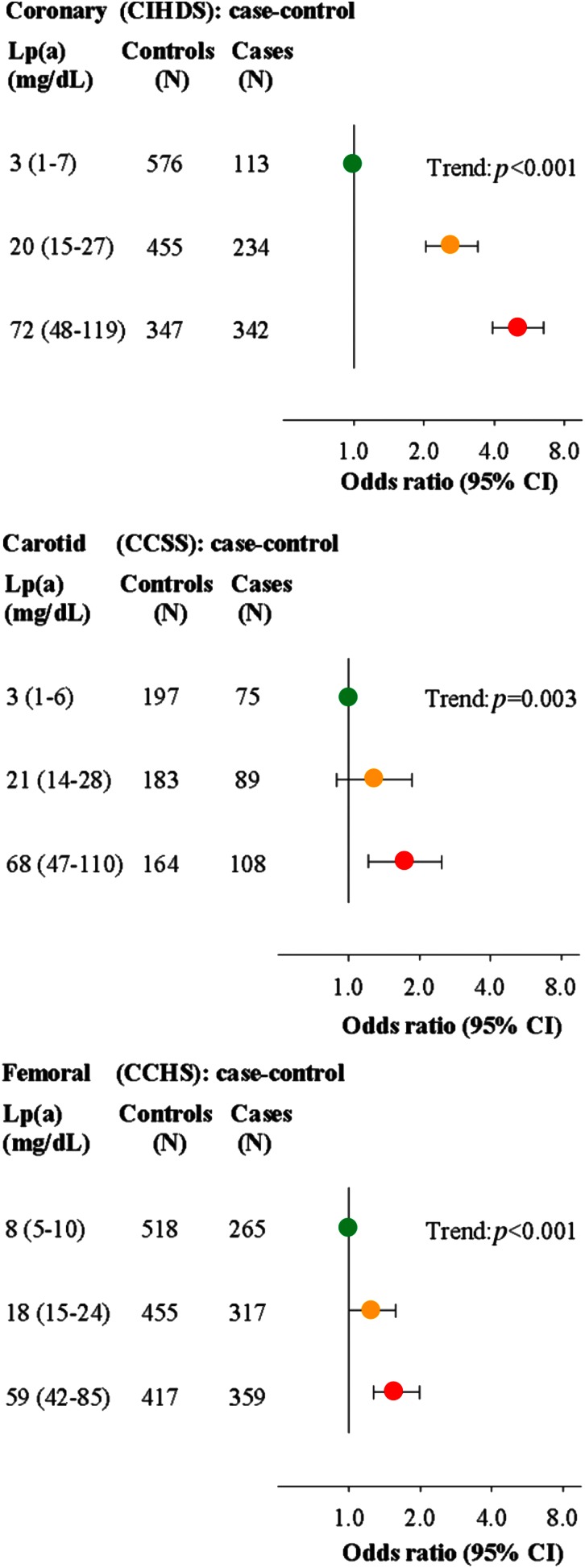
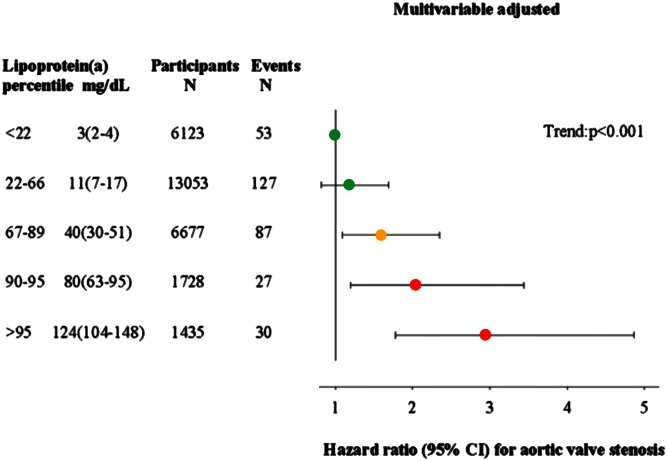
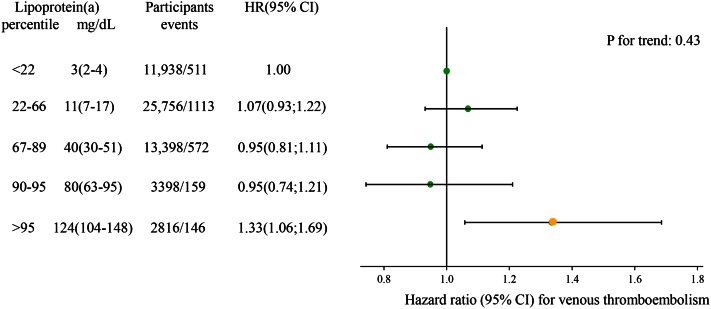
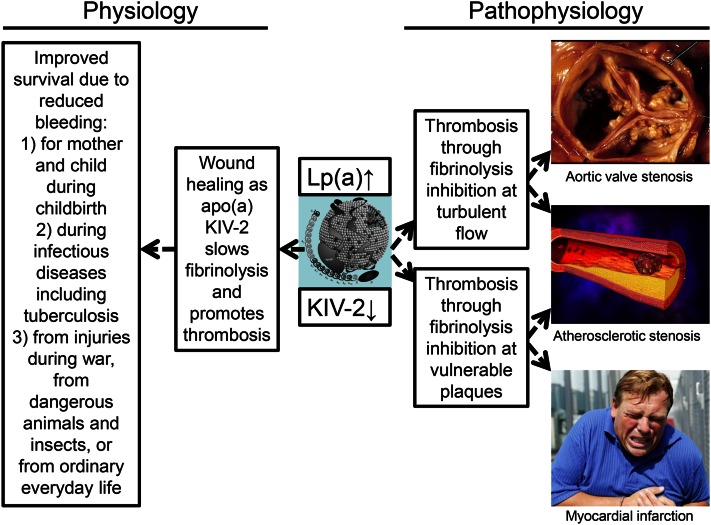
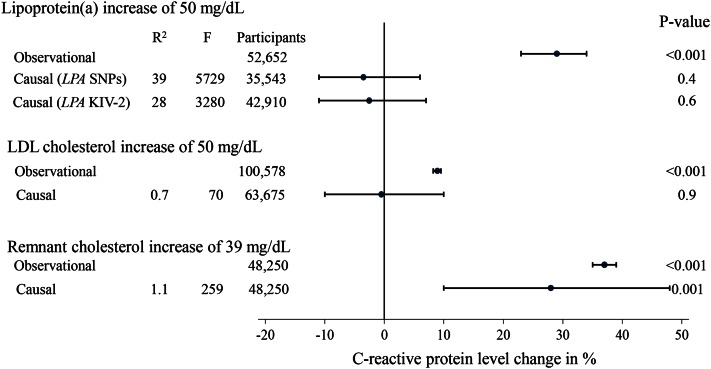
Human epidemiologic and genetic evidence using the Mendelian randomization approach in large-scale studies now strongly supports that elevated lipoprotein (a) [Lp(a)] is a causal risk factor for cardiovascular disease, that is, for myocardial infarction, atherosclerotic stenosis, and aortic valve stenosis. The Mendelian randomization approach used to infer causality is generally not affected by confounding and reverse causation, the major problems of observational epidemiology. This approach is particularly valuable to study causality of Lp(a), as single genetic variants exist that explain 27-28% of all variation in plasma Lp(a). The most important genetic variant likely is the kringle IV type 2 (KIV-2) copy number variant, as the apo(a) product of this variant influences fibrinolysis and thereby thrombosis, as opposed to the Lp(a) particle per se. We speculate that the physiological role of KIV-2 in Lp(a) could be through wound healing during childbirth, infections, and injury, a role that, in addition, could lead to more blood clots promoting stenosis of arteries and the aortic valve, and myocardial infarction. Randomized placebo-controlled trials of Lp(a) reduction in individuals with very high concentrations to reduce cardiovascular disease are awaited. Recent genetic evidence documents elevated Lp(a) as a cause of myocardial infarction, atherosclerotic stenosis, and aortic valve stenosis.
Keywords: apolipoproteins; atherosclerosis; cholesterol; dyslipidemias; inflammation; lipids; low density lipoprotein; plasminogen; vascular biology.
Copyright © 2016 by the American Society for Biochemistry and Molecular Biology, Inc.
Figures
References
-
- Berg, K. 1963. A new serum type system in man–the LP system. Acta Pathol. Microbiol. Scand. 59: 369–382. - PubMed
-
- Berg, K., and J. Mohr. 1963. Genetics of the LP system. Acta Genet. Stat. Med. 13: 349–360. - PubMed
-
- Mohr, J., and K. Berg. 1963. Genetics of the LP serum types: associations and linkage relations. Acta Genet. Stat. Med. 13: 343–348. - PubMed
-
- McLean J. W., Tomlinson J. E., Kuang W. J., Eaton D. L., Chen E. Y., Fless G. M., Scanu A. M., and Lawn R. M.. 1987. cDNA sequence of human apolipoprotein(a) is homologous to plasminogen. Nature. 330: 132–137. - PubMed
-
- Lawn R. M. 1992. Lipoprotein(a) in heart disease. Sci. Am. 266: 54–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
