

Pathophysiology of colorectal peritoneal carcinomatosis: Role of the peritoneum
- PMID: 27678351
- PMCID: PMC5016368
- DOI: 10.3748/wjg.v22.i34.7692
Pathophysiology of colorectal peritoneal carcinomatosis: Role of the peritoneum
Abstract
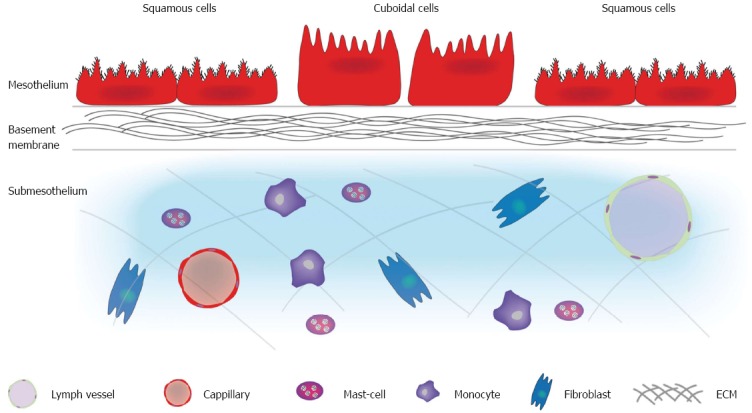
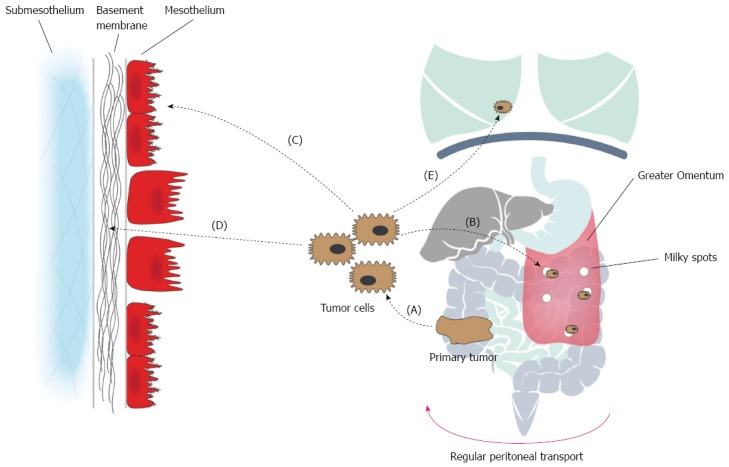
Colorectal cancer (CRC) is the third most common cancer and the fourth most common cause of cancer-related death worldwide. Besides the lymphatic and haematogenous routes of dissemination, CRC frequently gives rise to transcoelomic spread of tumor cells in the peritoneal cavity, which ultimately leads to peritoneal carcinomatosis (PC). PC is associated with a poor prognosis and bad quality of life for these patients in their terminal stages of disease. A loco-regional treatment modality for PC combining cytoreductive surgery and hyperthermic intraperitoneal peroperative chemotherapy has resulted in promising clinical results. However, this novel approach is associated with significant morbidity and mortality. A comprehensive understanding of the molecular events involved in peritoneal disease spread is paramount in avoiding unnecessary toxicity. The emergence of PC is the result of a molecular crosstalk between cancer cells and host elements, involving several well-defined steps, together known as the peritoneal metastatic cascade. Individual or clumps of tumor cells detach from the primary tumor, gain access to the peritoneal cavity and become susceptible to the regular peritoneal transport. They attach to the distant peritoneum, subsequently invade the subperitoneal space, where angiogenesis sustains proliferation and enables further metastatic growth. These molecular events are not isolated events but rather a continuous and interdependent process. In this manuscript, we review current data regarding the molecular mechanisms underlying the development of colorectal PC, with a special focus on the peritoneum and the role of the surgeon in peritoneal disease spread.
Keywords: Cytoreductive surgery; Hyperthermic intraperitoneal peroperative chemotherapy; Pathophysiology; Peritoneal carcinomatosis; Peritoneal metastatic cascade; Peritoneum.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interest for this article.
Figures
References
-
- Siegel R, Desantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin. 2014;64:104–117. - PubMed
-
- Easson AM, Bezjak A, Ross S, Wright JG. The ability of existing questionnaires to measure symptom change after paracentesis for symptomatic ascites. Ann Surg Oncol. 2007;14:2348–2357. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
