

Plastic Surgery Challenges in War Wounded II: Regenerative Medicine
- PMID: 27679752
- PMCID: PMC5028905
- DOI: 10.1089/wound.2015.0655
Plastic Surgery Challenges in War Wounded II: Regenerative Medicine
Abstract
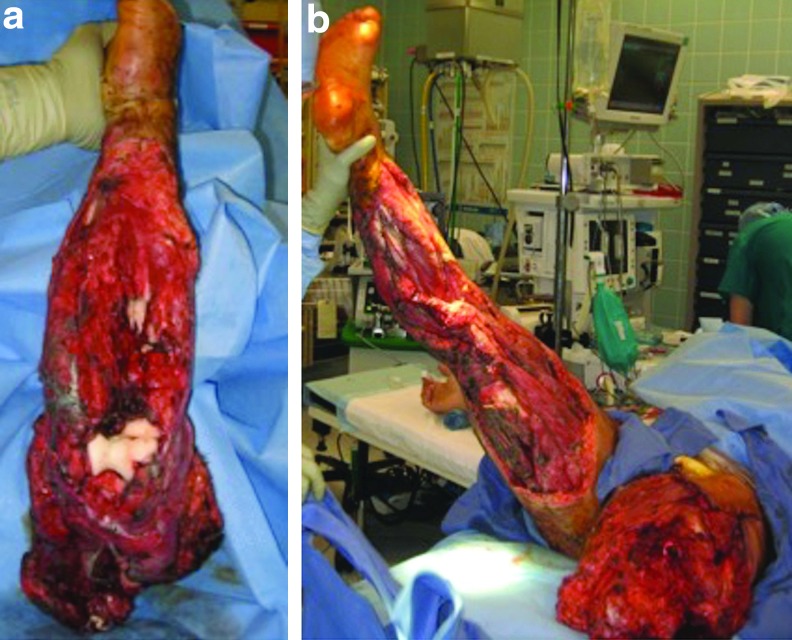
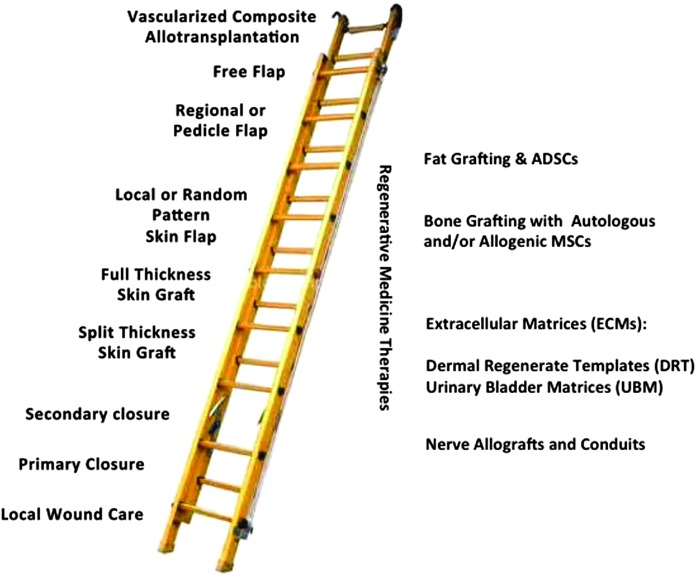
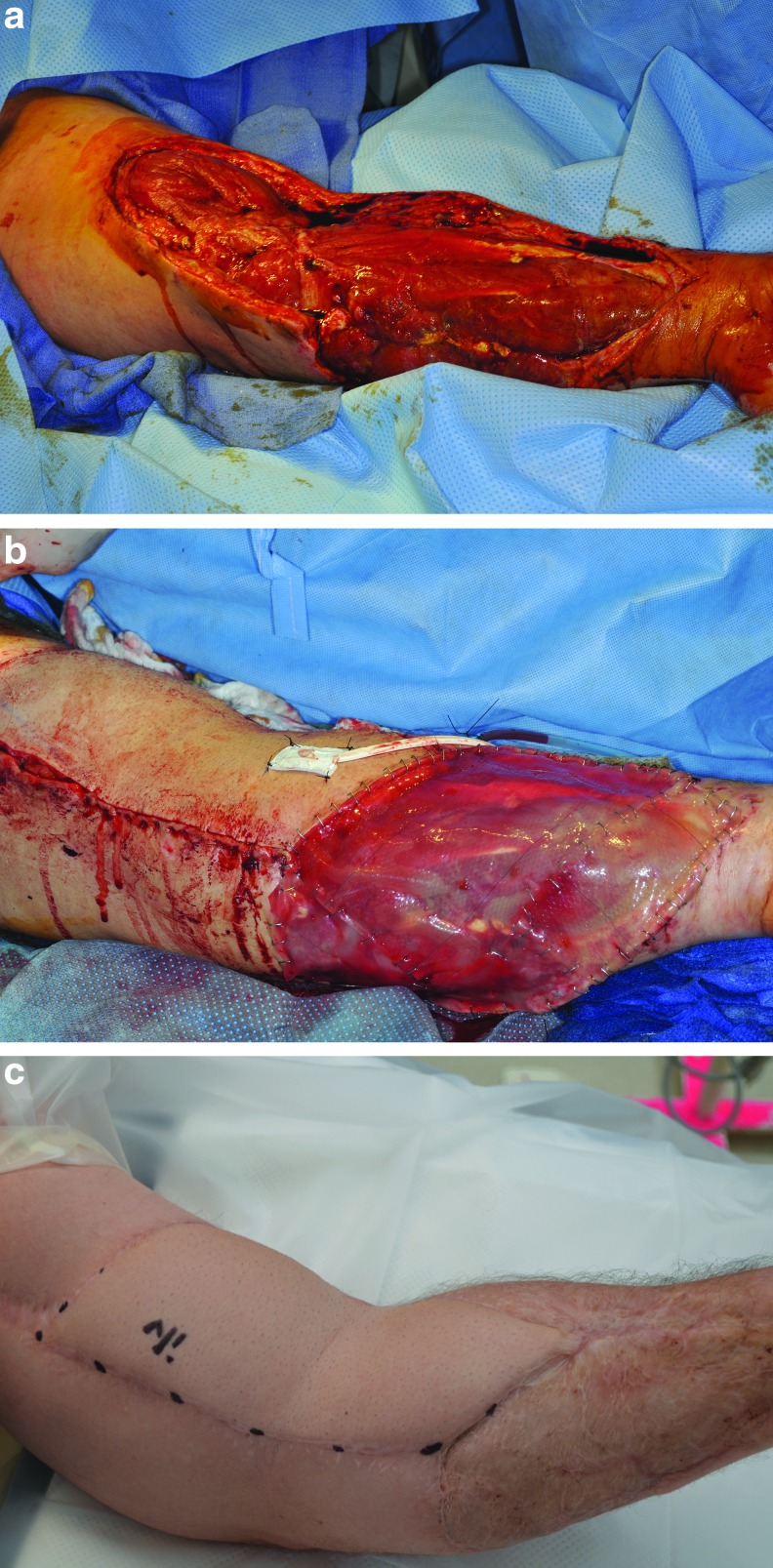
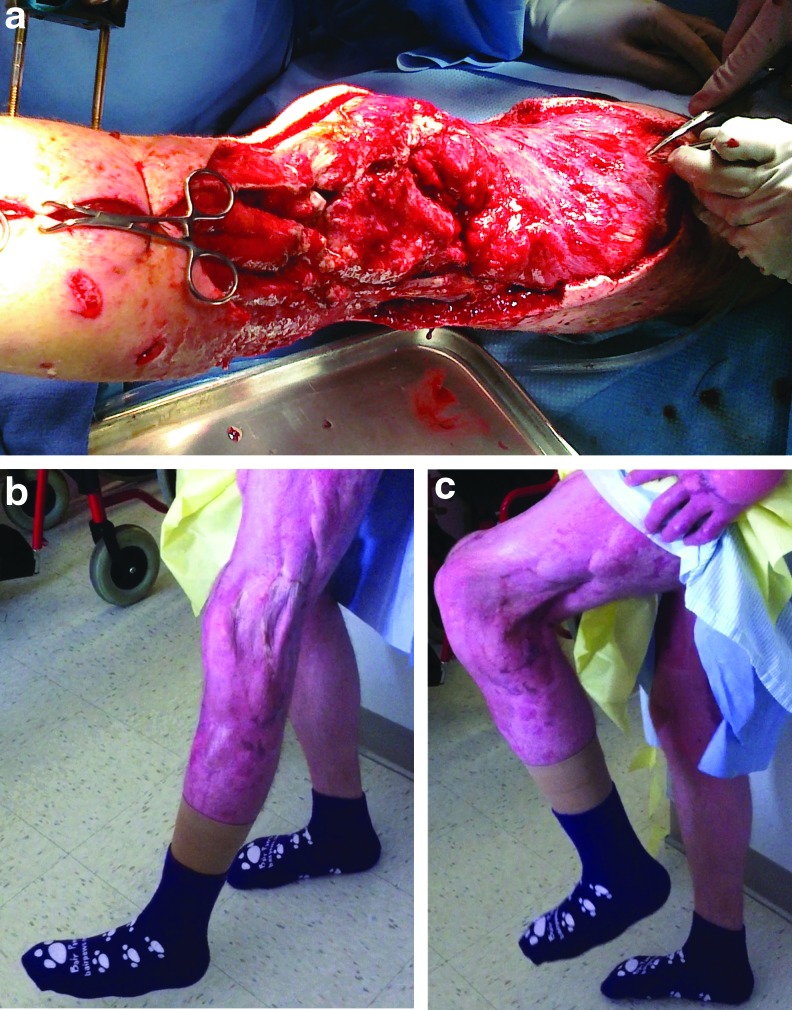
Background: A large volume of service members have sustained complex injuries during Operations Iraqi Freedom (OIF) and Enduring Freedom (OEF). These injuries are complicated by contamination with particulate and foreign materials, have high rates of bacterial and/or fungal infections, are often composite-type defects with massive soft tissue wounds, and usually have multisystem involvement. While traditional treatment modalities remain a mainstay for optimal wound care, traditional reconstruction approaches alone may be inadequate to fully address the scope and magnitude of such massive complex wounds. As a result of these difficult clinical problems, the use of regenerative medicine therapies, such as autologous adipose tissue grafting, stem cell therapies, nerve allografts, and dermal regenerate templates/extracellular matrix scaffolds, is increased as adjuncts to traditional reconstructive measures. Basic and Clinical Science Advances: The beneficial applications of regenerative medicine therapies have been well characterized in both in vitro studies and in vivo animal studies. The use of these regenerative medicine techniques in the treatment of combat casualty injuries has been increasing throughout the recent war conflicts. Clinical Care Relevance: Military medicine has shown positive results when utilizing certain regenerative medicine modalities in treating complex war wounds. As a result, multi-institution clinical trials are underway to further evaluate these observations and reconstruction measures. Conclusion: Successful combat casualty wound care often requires a combination of traditional aspects of the reconstructive ladder/elevator with adoption of various regenerative medicine therapies. Due to the recent OIF/OEF conflicts, a high volume of combat casualties have benefited from adoption of regenerative medicine therapies and increased access to innovative clinical trials. Furthermore, many of these patients have had long-term follow-up to report on clinical outcomes that substantiate current treatment paradigms and concepts within regenerative medicine, reconstructive, and rehabilitation care. These results are applicable to not only combat casualty care but also to nonmilitary patients.
Keywords: complex wound care; limb salvage; regenerative medicine; war trauma.
Conflict of interest statement
Author Disclosure and Ghostwriting The authors have no affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the article. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. The views expressed in this presentation are those of the authors and do not necessarily reflect the official policy or position of the Department of Army, Department of Defense, or the U.S. Government.
Figures

Similar articles
-
Plastic Surgery Challenges in War Wounded I: Flap-Based Extremity Reconstruction.Adv Wound Care (New Rochelle). 2016 Sep 1;5(9):403-411. doi: 10.1089/wound.2015.0656. Adv Wound Care (New Rochelle). 2016. PMID: 27679751 Free PMC article. Review.
-
Regenerative medicine applications in combat casualty care.Regen Med. 2014 Mar;9(2):179-90. doi: 10.2217/rme.13.96. Regen Med. 2014. PMID: 24750059 Review.
-
Burns sustained in combat explosions in Operations Iraqi and Enduring Freedom (OIF/OEF explosion burns).Burns. 2006 Nov;32(7):853-7. doi: 10.1016/j.burns.2006.03.008. Epub 2006 Aug 8. Burns. 2006. PMID: 16899341
-
Rehabilitation needs of combat-injured service members admitted to the VA Polytrauma Rehabilitation Centers: the role of PM&R in the care of wounded warriors.PM R. 2009 Jan;1(1):23-8. doi: 10.1016/j.pmrj.2008.10.003. PM R. 2009. PMID: 19627869
-
[Epidemiology of war injuries, about two conflicts: Iraq and Afghanistan].Ann Fr Anesth Reanim. 2011 Nov;30(11):819-27. doi: 10.1016/j.annfar.2011.05.018. Epub 2011 Oct 5. Ann Fr Anesth Reanim. 2011. PMID: 21981845 Review. French.
Cited by
-
Free Tissue Transfer Versus Locoregional Flaps for the Reconstruction of Small and Moderate Defects in the Head and Neck Region: A Narrative Review.Cureus. 2025 May 23;17(5):e84711. doi: 10.7759/cureus.84711. eCollection 2025 May. Cureus. 2025. PMID: 40557032 Free PMC article. Review.
-
Holistic Approach of Swiss Fetal Progenitor Cell Banking: Optimizing Safe and Sustainable Substrates for Regenerative Medicine and Biotechnology.Front Bioeng Biotechnol. 2020 Oct 23;8:557758. doi: 10.3389/fbioe.2020.557758. eCollection 2020. Front Bioeng Biotechnol. 2020. PMID: 33195124 Free PMC article.
References
-
- Zouris JM, Walter GJ, Dye J, Galarneau M. Wounding patterns for U.S. marines and sailors during operation Iraqui freedom, major combat phase. Mil Med 2006;171:246–252 - PubMed
-
- Ramasamy A, Hill AM, Clasper JC. Improvised explosive devices: pathophysiology, injury profiles and current medical management. J R Army Med Corps 2009;155:265–272 - PubMed
-
- Shen-Gunther J, Ellison R, Kuhens C, Roach CJ, Jarrard S. Trends in combat casualty care by forward surgical teams deployed to Afghanistan. Mil Med 2011;176:67–78 - PubMed
-
- Valerio IL, Sabino J, Mundinger GS, Kumar A. From battleside to stateside: the reconstructive journey of our wounded warriors. Ann Plast Surg 2014;72 Suppl 1:S38–S45 - PubMed
-
- Kumar AR, Grewal NS, Chung TL, Bradley JP. Lessons from operation Iraqi freedom: successful subacute reconstruction of complex lower extremity battle injuries. Plast Reconstr Surg 2009;123:218–229 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
