

Staphylococcus capitis isolated from prosthetic joint infections
- PMID: 27680718
- PMCID: PMC5203848
- DOI: 10.1007/s10096-016-2777-7
Staphylococcus capitis isolated from prosthetic joint infections
Abstract
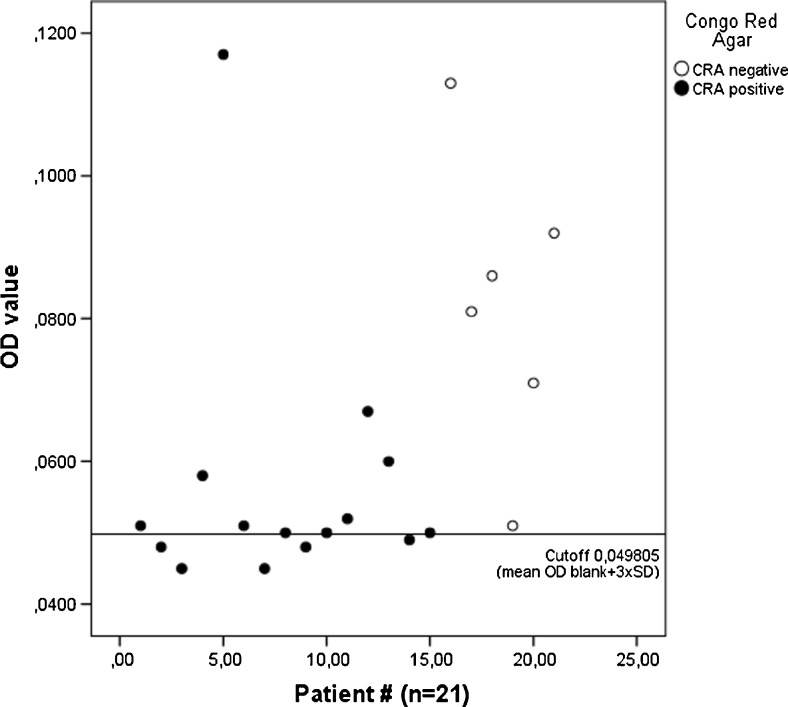
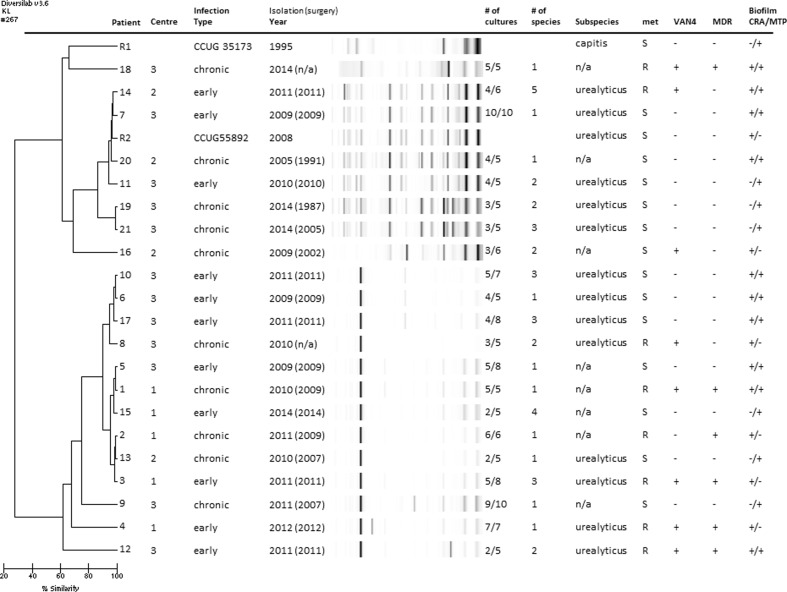
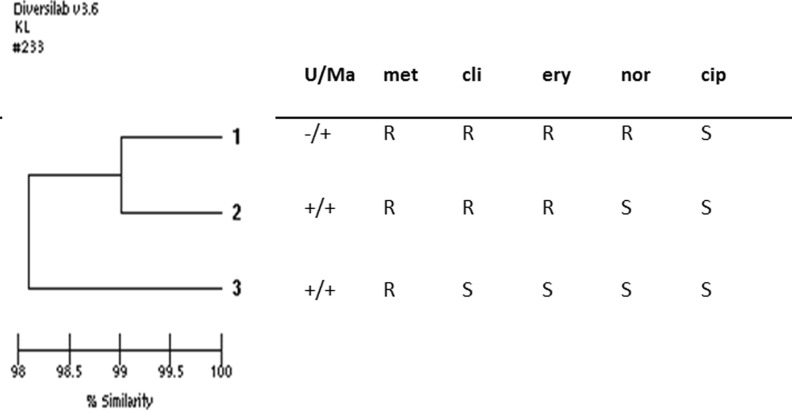
Further knowledge about the clinical and microbiological characteristics of prosthetic joint infections (PJIs) caused by different coagulase-negative staphylococci (CoNS) may facilitate interpretation of microbiological findings and improve treatment algorithms. Staphylococcus capitis is a CoNS with documented potential for both human disease and nosocomial spread. As data on orthopaedic infections are scarce, our aim was to describe the clinical and microbiological characteristics of PJIs caused by S. capitis. This retrospective cohort study included three centres and 21 patients with significant growth of S. capitis during revision surgery for PJI between 2005 and 2014. Clinical data were extracted and further microbiological characterisation of the S. capitis isolates was performed. Multidrug-resistant (≥3 antibiotic groups) S. capitis was detected in 28.6 % of isolates, methicillin resistance in 38.1 % and fluoroquinolone resistance in 14.3 %; no isolates were rifampin-resistant. Heterogeneous glycopeptide-intermediate resistance was detected in 38.1 %. Biofilm-forming ability was common. All episodes were either early post-interventional or chronic, and there were no haematogenous infections. Ten patients experienced monomicrobial infections. Among patients available for evaluation, 86 % of chronic infections and 70 % of early post-interventional infections achieved clinical cure; 90 % of monomicrobial infections remained infection-free. Genetic fingerprinting with repetitive sequence-based polymerase chain reaction (rep-PCR; DiversiLab®) displayed clustering of isolates, suggesting that nosocomial spread might be present. Staphylococcus capitis has the potential to cause PJIs, with infection most likely being contracted during surgery or in the early postoperative period. As S. capitis might be an emerging nosocomial pathogen, surveillance of the prevalence of PJIs caused by S. capitis could be recommended.
Conflict of interest statement
Compliance with ethical standardsFundingThis work was supported by grants from the research committee of Värmland County Council, Sweden (grant numbers LIVFOU-456821 and LIVFOU-457061), from the research committee of Östergötland County Council, Sweden (grant number LIO-447091) and from Örebro University, Sweden (ORU 1.3.1-01273/2015).Conflict of interestBo Söderquist has been a consultant for Pfizer and Janssen-Cilag. Åsa Nilsdotter-Augustinsson is a member of the expert group in the field of primary immunodeficiency for Baxalta Sweden AB. All other authors declare no conflicts of interest.
Figures
References
-
- Osmon DR, Berbari EF, Berendt AR, Lew D, Zimmerli W, Steckelberg JM, Rao N, Hanssen A, Wilson WR, Infectious Diseases Society of America Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2013;56(1):e1–e25. doi: 10.1093/cid/cis803. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
