

Diffusion Tractography of the Entire Left Ventricle by Using Free-breathing Accelerated Simultaneous Multisection Imaging
- PMID: 27681278
- PMCID: PMC5318239
- DOI: 10.1148/radiol.2016152613
Diffusion Tractography of the Entire Left Ventricle by Using Free-breathing Accelerated Simultaneous Multisection Imaging
Abstract
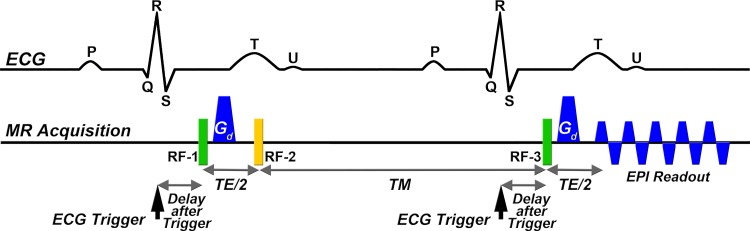
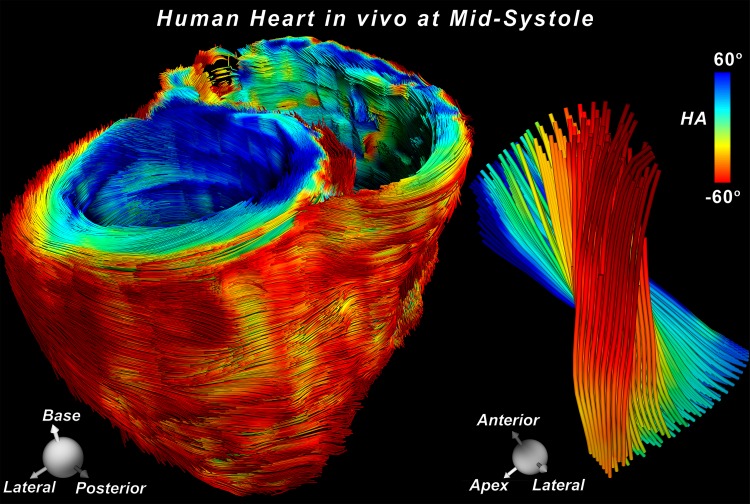
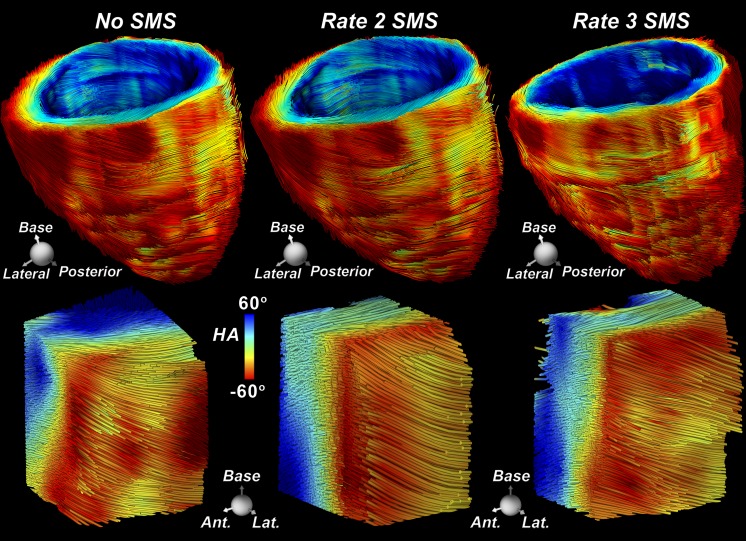
Purpose To develop a clinically feasible whole-heart free-breathing diffusion-tensor (DT) magnetic resonance (MR) imaging approach with an imaging time of approximately 15 minutes to enable three-dimensional (3D) tractography. Materials and Methods The study was compliant with HIPAA and the institutional review board and required written consent from the participants. DT imaging was performed in seven healthy volunteers and three patients with pulmonary hypertension by using a stimulated echo sequence. Twelve contiguous short-axis sections and six four-chamber sections that covered the entire left ventricle were acquired by using simultaneous multisection (SMS) excitation with a blipped-controlled aliasing in parallel imaging readout. Rate 2 and rate 3 SMS excitation was defined as two and three times accelerated in the section axis, respectively. Breath-hold and free-breathing images with and without SMS acceleration were acquired. Diffusion-encoding directions were acquired sequentially, spatiotemporally registered, and retrospectively selected by using an entropy-based approach. Myofiber helix angle, mean diffusivity, fractional anisotropy, and 3D tractograms were analyzed by using paired t tests and analysis of variance. Results No significant differences (P > .63) were seen between breath-hold rate 3 SMS and free-breathing rate 2 SMS excitation in transmural myofiber helix angle, mean diffusivity (mean ± standard deviation, [0.89 ± 0.09] × 10-3 mm2/sec vs [0.9 ± 0.09] × 10-3 mm2/sec), or fractional anisotropy (0.43 ± 0.05 vs 0.42 ± 0.06). Three-dimensional tractograms of the left ventricle with no SMS and rate 2 and rate 3 SMS excitation were qualitatively similar. Conclusion Free-breathing DT imaging of the entire human heart can be performed in approximately 15 minutes without section gaps by using SMS excitation with a blipped-controlled aliasing in parallel imaging readout, followed by spatiotemporal registration and entropy-based retrospective image selection. This method may lead to clinical translation of whole-heart DT imaging, enabling broad application in patients with cardiac disease. © RSNA, 2016 Online supplemental material is available for this article.
Figures
Comment in
-
Faster Diffusion-weighted MR Imaging of Cardiac Microstructure.Radiology. 2017 Mar;282(3):622-626. doi: 10.1148/radiol.2016162269. Radiology. 2017. PMID: 28218885 No abstract available.
References
-
- Reese TG, Weisskoff RM, Smith RN, Rosen BR, Dinsmore RE, Wedeen VJ. Imaging myocardial fiber architecture in vivo with magnetic resonance. Magn Reson Med 1995;34(6):786–791. - PubMed
-
- Gamper U, Boesiger P, Kozerke S. Diffusion imaging of the in vivo heart using spin echoes—considerations on bulk motion sensitivity. Magn Reson Med 2007;57(2):331–337. - PubMed
-
- Tseng WY, Reese TG, Weisskoff RM, Wedeen VJ. Cardiac diffusion tensor MRI in vivo without strain correction. Magn Reson Med 1999;42(2):393–403. - PubMed
-
- Wu MT, Su MY, Huang YL, et al. . Sequential changes of myocardial microstructure in patients postmyocardial infarction by diffusion-tensor cardiac MR: correlation with left ventricular structure and function. Circ Cardiovasc Imaging 2009;2(1):32–40, 6, 40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
