

The Spectrum of Histologic Findings in Hepatic Outflow Obstruction
- PMID: 27681331
- PMCID: PMC6420777
- DOI: 10.5858/arpa.2015-0388-OA
The Spectrum of Histologic Findings in Hepatic Outflow Obstruction
Abstract
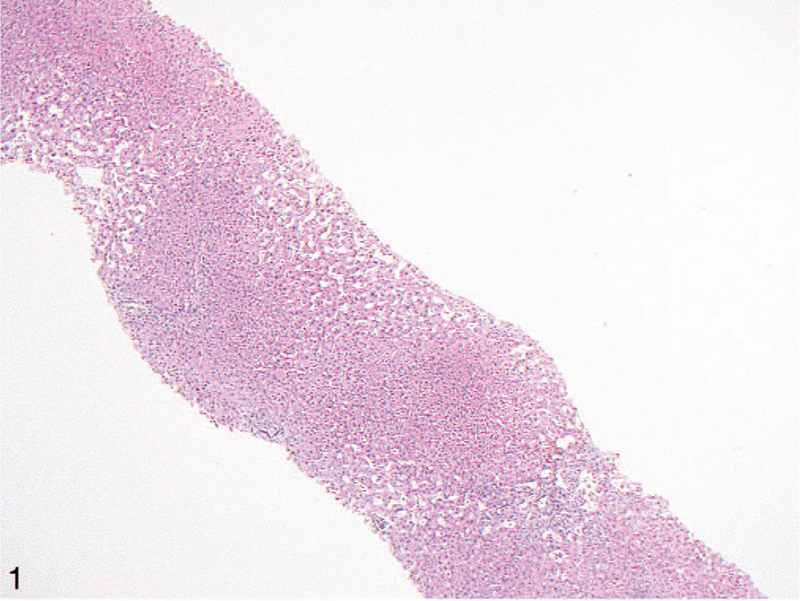
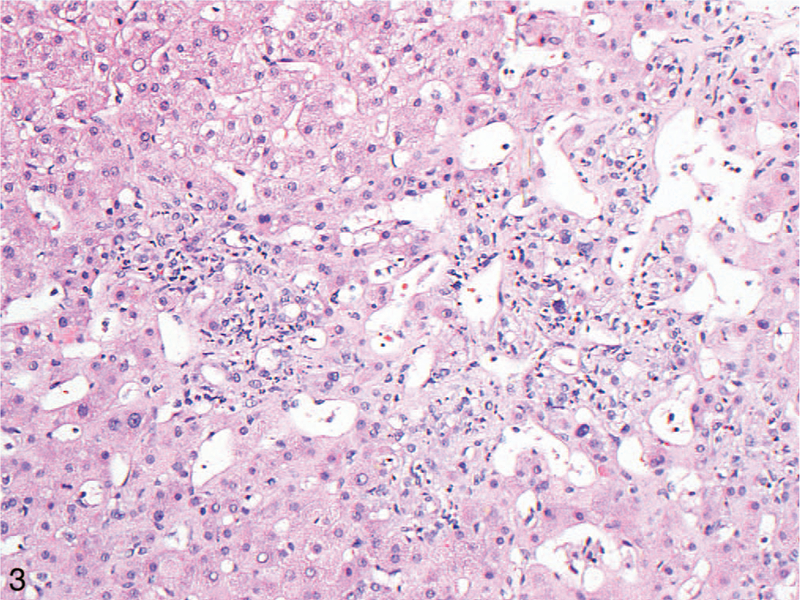
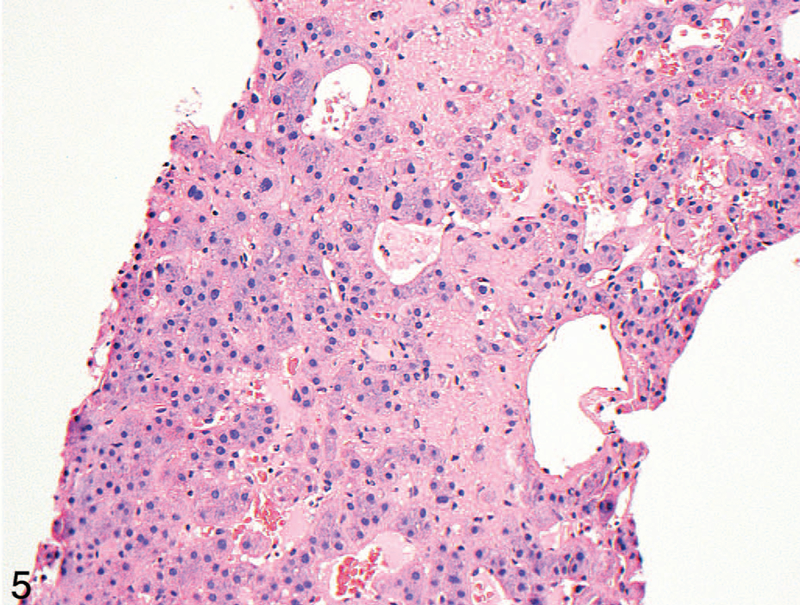
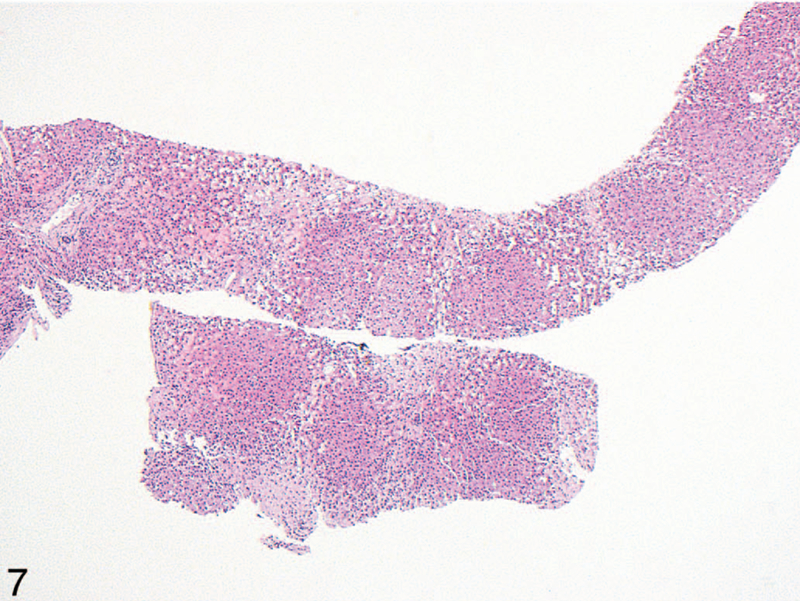
Context: -Cardiac hepatopathy and Budd-Chiari syndrome are 2 forms of hepatic venous outflow obstruction with different pathophysiology but overlapping histologic findings, including sinusoidal dilation and centrilobular necrosis.
Objective: -To determine whether a constellation of morphologic findings could help distinguish between the 2 and could suggest the diagnoses in previously undiagnosed patients.
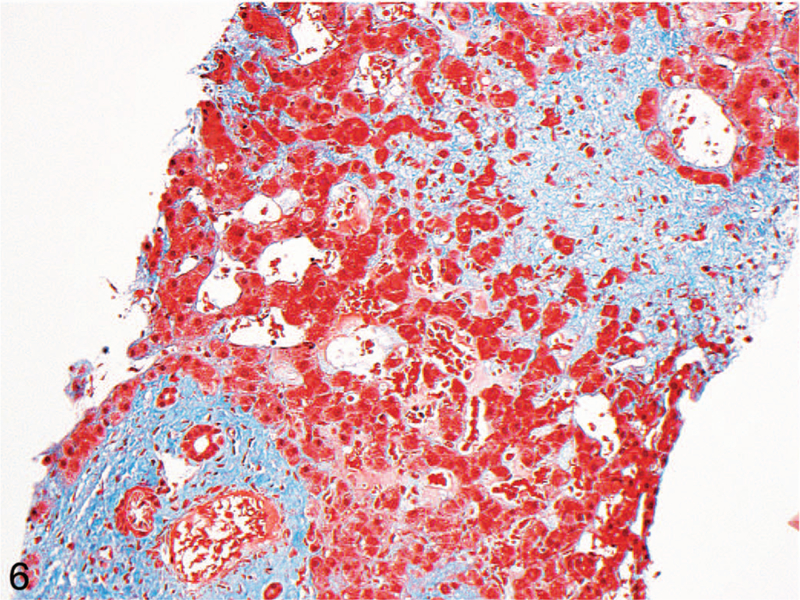
Design: -We identified 26 specimens with a diagnosis of cardiac hepatopathy and 23 with a diagnosis of Budd-Chiari syndrome. Slides stained with hematoxylin and eosin and with trichrome were evaluated for several distinctive histologic findings.
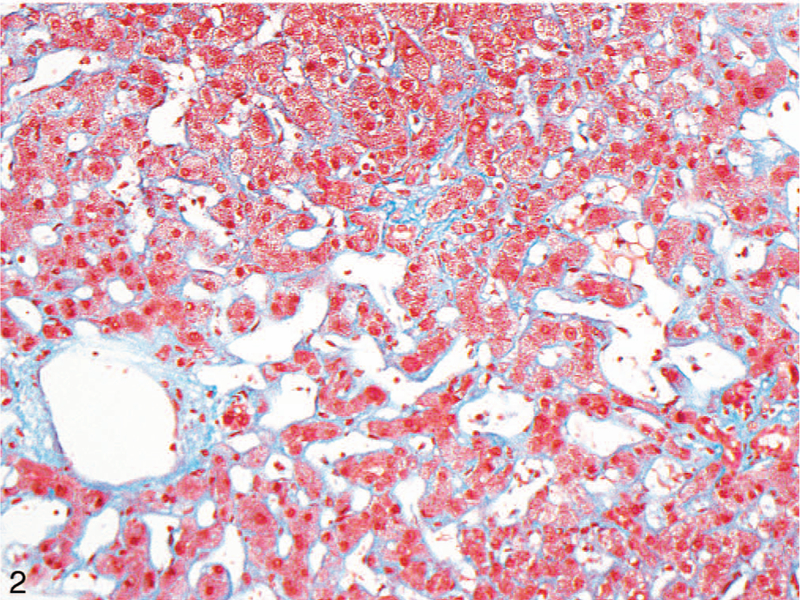
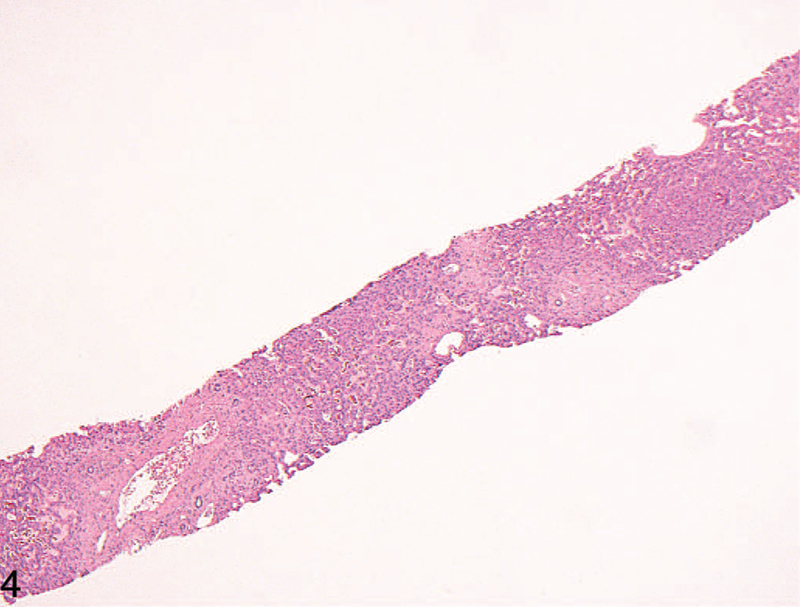
Results: -Features common to both forms of hepatic outflow obstruction included sinusoidal dilation and portal tract changes of fibrosis, chronic inflammation, and bile ductular reaction. Histologic findings significantly more common in cardiac hepatopathy included pericellular/sinusoidal fibrosis and fibrosis around the central vein. Only centrilobular hepatocyte dropout/necrosis was significantly more common in Budd-Chiari, regardless of duration.
Conclusions: -The finding of pericellular/sinusoidal fibrosis in cardiac hepatopathy compared with Budd-Chiari is not unexpected, given the chronic nature of most cardiac hepatopathy. Portal tract changes are common in both forms of hepatic outflow obstruction and should not deter one from making the diagnosis of hepatic outflow obstruction. Fibrosis along sinusoids and around the central vein may be suggestive of cardiac hepatopathy in biopsies from patients without a prior diagnosis.
Conflict of interest statement
The authors have no relevant financial interest in the products or companies described in this article.
Figures
References
-
- Valla DC. Primary Budd-Chiari syndrome. J Hepatol 2009;50(1):195–203. - PubMed
-
- Cazals-Hatem D, Vilgrain V, Genin P, et al. Arterial and portal circulation and parenchymal changes in Budd-Chiari syndrome: a study in 17 explanted livers. Hepatology 2003;37(3):510–519. - PubMed
-
- Hsu RB, Chang CI, Lin FY, et al. Heart transplantation in patients with liver cirrhosis. Eur J Cardiothorac Surg 2008;34(2):307–312. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical