

A Prospective Clinical Trial Combining Radiation Therapy With Systemic Immunotherapy in Metastatic Melanoma
- PMID: 27681753
- PMCID: PMC5077166
- DOI: 10.1016/j.ijrobp.2016.07.005
A Prospective Clinical Trial Combining Radiation Therapy With Systemic Immunotherapy in Metastatic Melanoma
Abstract
Purpose: Local radiation therapy (RT) combined with systemic anti-cytotoxic T-lymphocyte-associated protein-4 immunotherapy may enhance induction of systemic antimelanoma immune responses. The primary objective of the present trial was to assess the safety and efficacy of combining ipilimumab with RT in patients with stage IV melanoma. The secondary objectives included laboratory assessment of induction of antimelanoma immune responses.
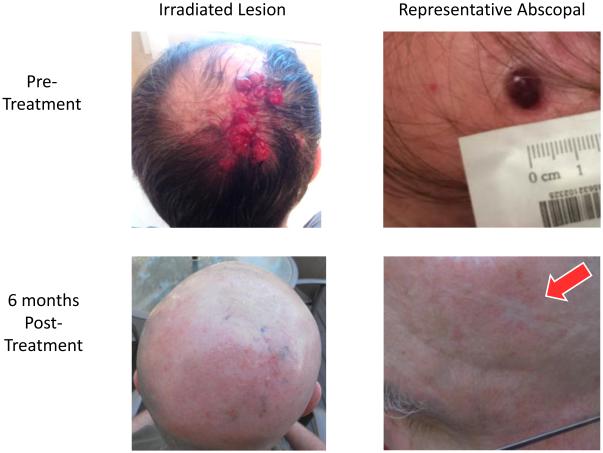
Methods and materials: In our prospective clinical trial, 22 patients with stage IV melanoma were treated with palliative RT and ipilimumab for 4 cycles. RT to 1 to 2 disease sites was initiated within 5 days after starting ipilimumab. Patients had ≥1 nonirradiated metastasis measuring ≥1.5 cm available for response assessment. Tumor imaging studies were obtained at baseline, 2 to 4 weeks after cycle 4 of ipilimumab, and every 3 months until progression. Laboratory immune response parameters were measured before and during treatment.
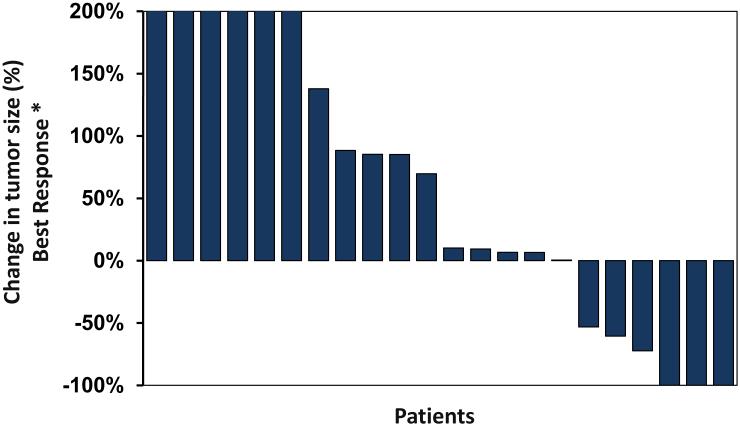
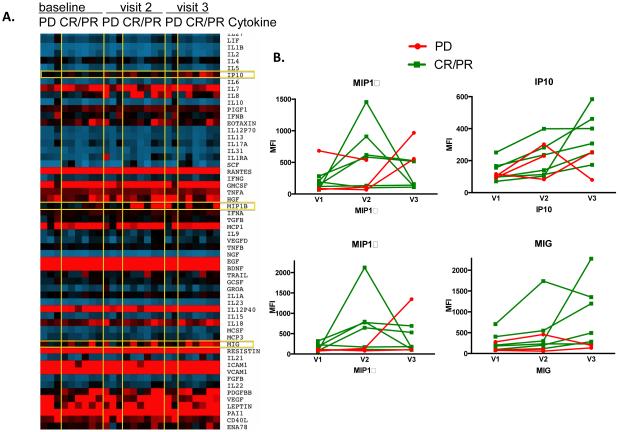
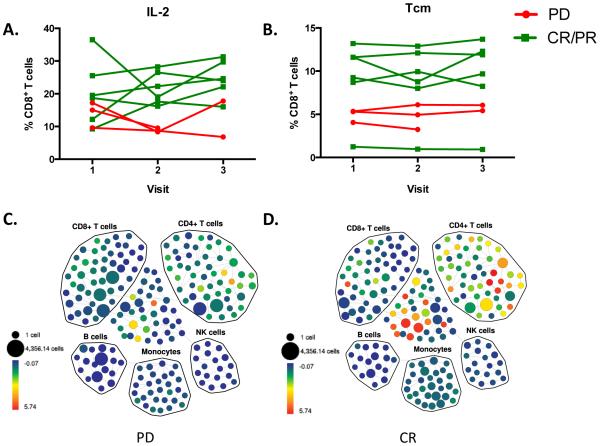
Results: Combination therapy was well-tolerated without unexpected toxicities. Eleven patients (50.0%) experienced clinical benefit from therapy, including complete and partial responses and stable disease at median follow-up of 55 weeks. Three patients (27.3%) achieved an ongoing systemic complete response at a median follow-up of 55 weeks (range 32-65), and 3 (27.3%) had an initial partial response for a median of 40 weeks. Analysis of immune response data suggested a relationship between elevated CD8-activated T-cells and response.
Conclusion: This is the second prospective clinical trial of treatment of metastatic melanoma using the combination of RT and systemic immunotherapy and the first using this sequence of therapy. The results from the present trial demonstrate that a subset of patients may benefit from combination therapy, arguing for continued clinical investigation of the use of RT combined with immunotherapy, including programmed cell death 1 inhibitors, which might have the potential to be even more effective in combination with RT.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Barrow C, et al. Tumor antigen expression in melanoma varies according to antigen and stage. Clin Cancer Res. 2006;12(3):764–71. Pt 1. - PubMed
-
- Clemente CG, et al. Prognostic value of tumor infiltrating lymphocytes in the vertical growth phase of primary cutaneous melanoma. Cancer. 1996;77(7):1303–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
