

Adjunctive Azithromycin Prophylaxis for Cesarean Delivery
- PMID: 27682034
- PMCID: PMC5131636
- DOI: 10.1056/NEJMoa1602044
Adjunctive Azithromycin Prophylaxis for Cesarean Delivery
Abstract
Background: The addition of azithromycin to standard regimens for antibiotic prophylaxis before cesarean delivery may further reduce the rate of postoperative infection. We evaluated the benefits and safety of azithromycin-based extended-spectrum prophylaxis in women undergoing nonelective cesarean section.
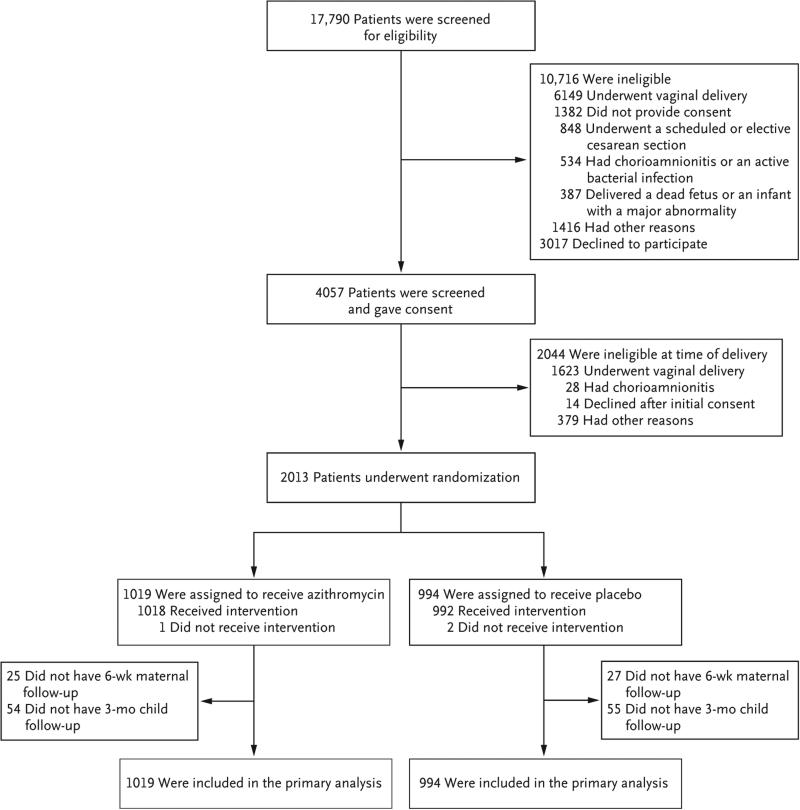
Methods: In this trial conducted at 14 centers in the United States, we studied 2013 women who had a singleton pregnancy with a gestation of 24 weeks or more and who were undergoing cesarean delivery during labor or after membrane rupture. We randomly assigned 1019 to receive 500 mg of intravenous azithromycin and 994 to receive placebo. All the women were also scheduled to receive standard antibiotic prophylaxis. The primary outcome was a composite of endometritis, wound infection, or other infection occurring within 6 weeks.
Results: The primary outcome occurred in 62 women (6.1%) who received azithromycin and in 119 (12.0%) who received placebo (relative risk, 0.51; 95% confidence interval [CI], 0.38 to 0.68; P<0.001). There were significant differences between the azithromycin group and the placebo group in rates of endometritis (3.8% vs. 6.1%, P=0.02), wound infection (2.4% vs. 6.6%, P<0.001), and serious maternal adverse events (1.5% vs. 2.9%, P=0.03). There was no significant between-group difference in a secondary neonatal composite outcome that included neonatal death and serious neonatal complications (14.3% vs. 13.6%, P=0.63).
Conclusions: Among women undergoing nonelective cesarean delivery who were all receiving standard antibiotic prophylaxis, extended-spectrum prophylaxis with adjunctive azithromycin was more effective than placebo in reducing the risk of postoperative infection. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; C/SOAP ClinicalTrials.gov number, NCT01235546 .).
Figures
Comment in
-
Antibiotic Prophylaxis for Cesarean Delivery - When Broader Is Better.N Engl J Med. 2016 Sep 29;375(13):1284-6. doi: 10.1056/NEJMe1610010. N Engl J Med. 2016. PMID: 27682038 No abstract available.
-
Adjunctive Azithromycin Prophylaxis for Cesarean Delivery.N Engl J Med. 2017 Jan 12;376(2):182. doi: 10.1056/NEJMc1614626. N Engl J Med. 2017. PMID: 28076707 No abstract available.
-
Adjunctive Azithromycin Prophylaxis for Cesarean Delivery.N Engl J Med. 2017 Jan 12;376(2):181. doi: 10.1056/NEJMc1614626. N Engl J Med. 2017. PMID: 28079334 No abstract available.
-
Adjunctive Azithromycin Prophylaxis for Cesarean Delivery.N Engl J Med. 2017 Jan 12;376(2):181-2. doi: 10.1056/NEJMc1614626. N Engl J Med. 2017. PMID: 28079335 No abstract available.
-
Implications of intrapartum azithromycin on neonatal microbiota.Lancet Infect Dis. 2017 Mar;17(3):253-254. doi: 10.1016/S1473-3099(17)30058-0. Epub 2017 Feb 23. Lancet Infect Dis. 2017. PMID: 28244378 No abstract available.
References
-
- Berg CJ, Chang J, Callaghan WM, Whitehead SJ. Pregnancy-related mortality in the United States, 1991-1997. Obstet Gynecol. 2003;101:289–96. - PubMed
-
- DeFrances CJ, Cullen KA, Kozak LJ. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat 13 2007. 165:1–209. - PubMed
-
- Gibbs RS. Clinical risk factors for puerperal infection. Obstet Gynecol. 1980;555(Suppl):178S–184S. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical