

Nonprogressing HIV-infected children share fundamental immunological features of nonpathogenic SIV infection
- PMID: 27683550
- PMCID: PMC6087524
- DOI: 10.1126/scitranslmed.aag1048
Nonprogressing HIV-infected children share fundamental immunological features of nonpathogenic SIV infection
Abstract
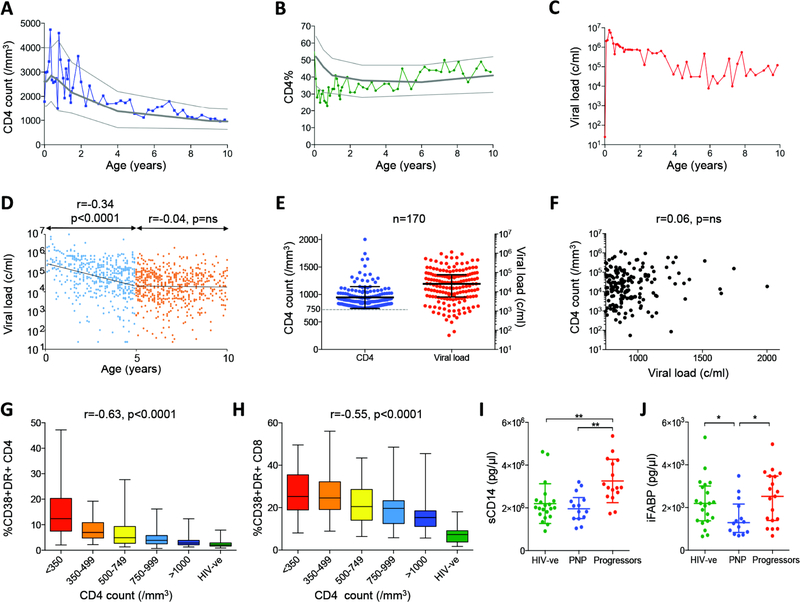
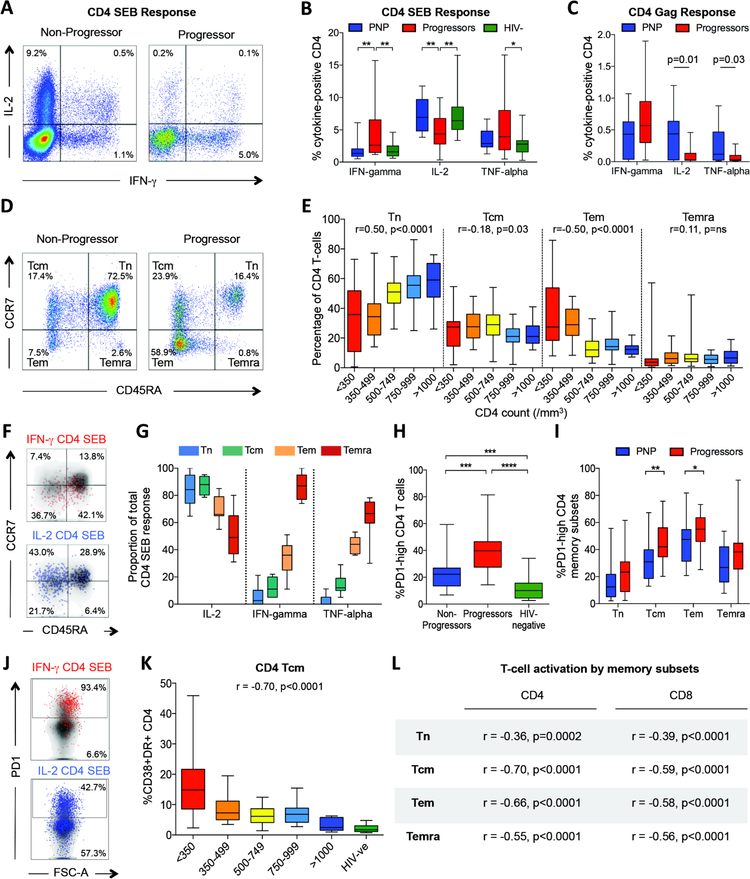
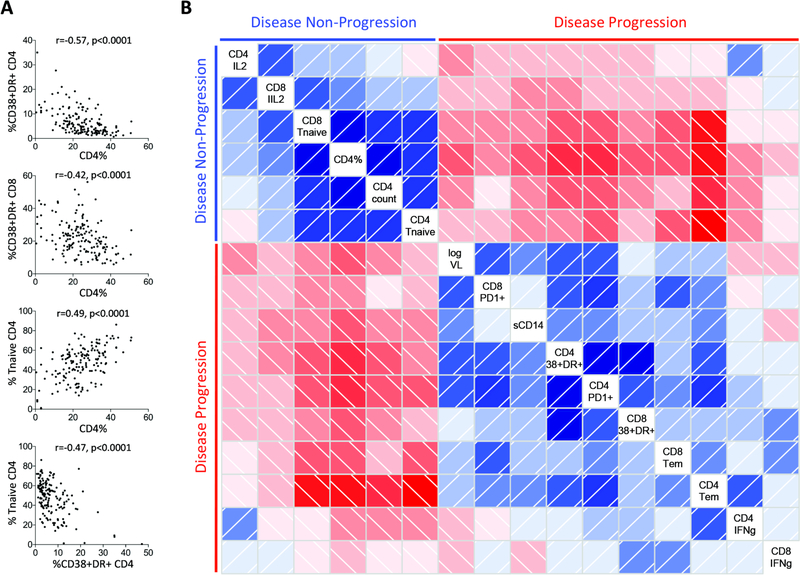
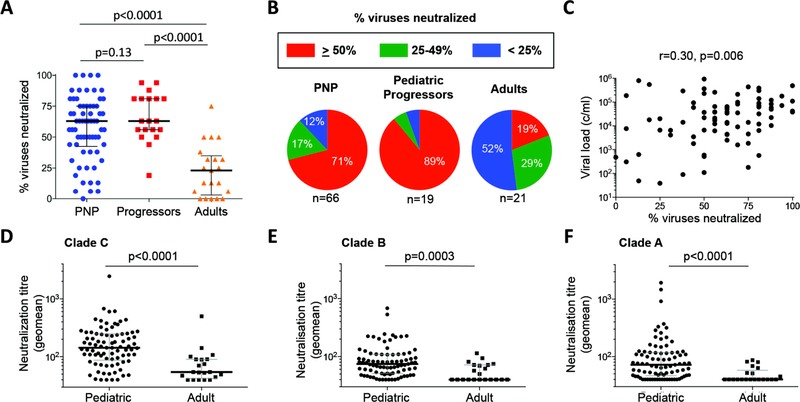
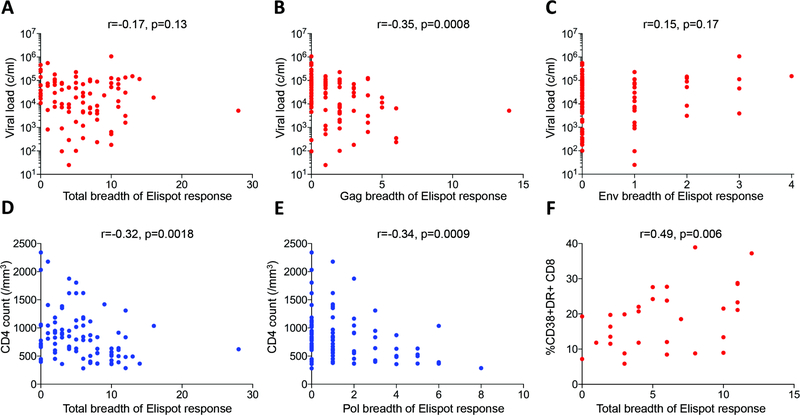
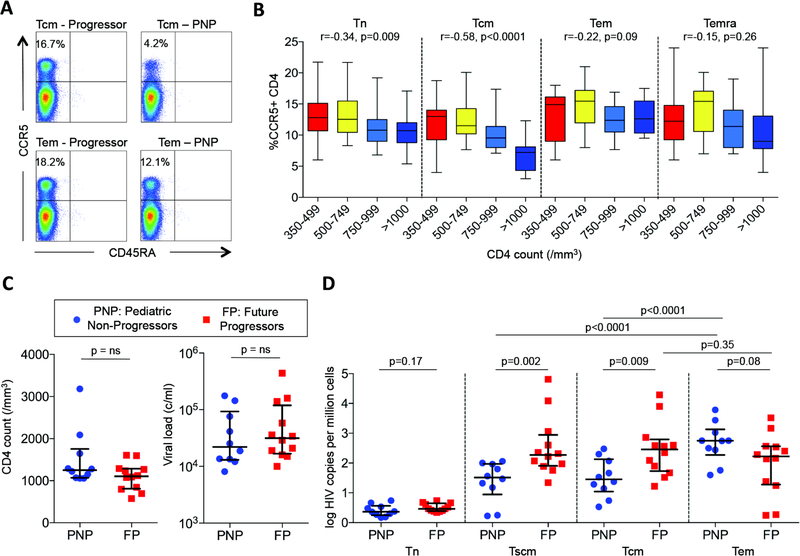
Disease-free infection in HIV-infected adults is associated with human leukocyte antigen-mediated suppression of viremia, whereas in the sooty mangabey and other healthy natural hosts of simian immunodeficiency virus (SIV), viral replication continues unabated. To better understand factors preventing HIV disease, we investigated pediatric infection, where AIDS typically develops more rapidly than in adults. Among 170 nonprogressing antiretroviral therapy-naïve children aged >5 years maintaining normal-for-age CD4 T cell counts, immune activation levels were low despite high viremia (median, 26,000 copies/ml). Potent, broadly neutralizing antibody responses in most of the subjects and strong virus-specific T cell activity were present but did not drive pediatric nonprogression. However, reduced CCR5 expression and low HIV infection in long-lived central memory CD4 T cells were observed in pediatric nonprogressors. These children therefore express two cardinal immunological features of nonpathogenic SIV infection in sooty mangabeys-low immune activation despite high viremia and low CCR5 expression on long-lived central memory CD4 T cells-suggesting closer similarities with nonpathogenetic mechanisms evolved over thousands of years in natural SIV hosts than those operating in HIV-infected adults.
Copyright © 2016, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
Do HIV-infected children who do not develop AIDS hold clues to a cure?AIDS. 2017 Jan 28;31(3):N4-N5. doi: 10.1097/QAD.0000000000001370. AIDS. 2017. PMID: 28002066 No abstract available.
References
-
- Hunt PW, Martin JN, Sinclair E, Bredt B, Hagos E, Lampiris H, Deeks SG, T cell activation is associated with lower CD4+ T cell gains in human immunodeficiency virus-infected patients with sustained viral suppression during antiretroviral therapy. The Journal of infectious diseases 187, 1534 (May 15, 2003). - PubMed
-
- Hunt PW, Brenchley J, Sinclair E, McCune JM, Roland M, Page-Shafer K, Hsue P, Emu B, Krone M, Lampiris H, Douek D, Martin JN, Deeks SG, Relationship between T cell activation and CD4+ T cell count in HIV-seropositive individuals with undetectable plasma HIV RNA levels in the absence of therapy. The Journal of infectious diseases 197, 126 (January 1, 2008). - PMC - PubMed
-
- Finkel TH, Tudor-Williams G, Banda NK, Cotton MF, Curiel T, Monks C, Baba TW, Ruprecht RM, Kupfer A, Apoptosis occurs predominantly in bystander cells and not in productively infected cells of HIV- and SIV-infected lymph nodes. Nature medicine 1, 129 (February, 1995). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
