

Hemodynamic evidence of vascular remodeling in combined post- and precapillary pulmonary hypertension
- PMID: 27683608
- PMCID: PMC5019084
- DOI: 10.1086/688516
Hemodynamic evidence of vascular remodeling in combined post- and precapillary pulmonary hypertension
Abstract
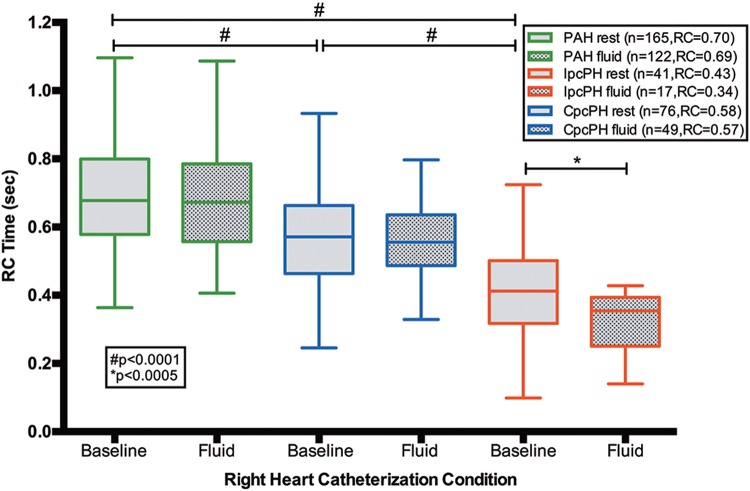
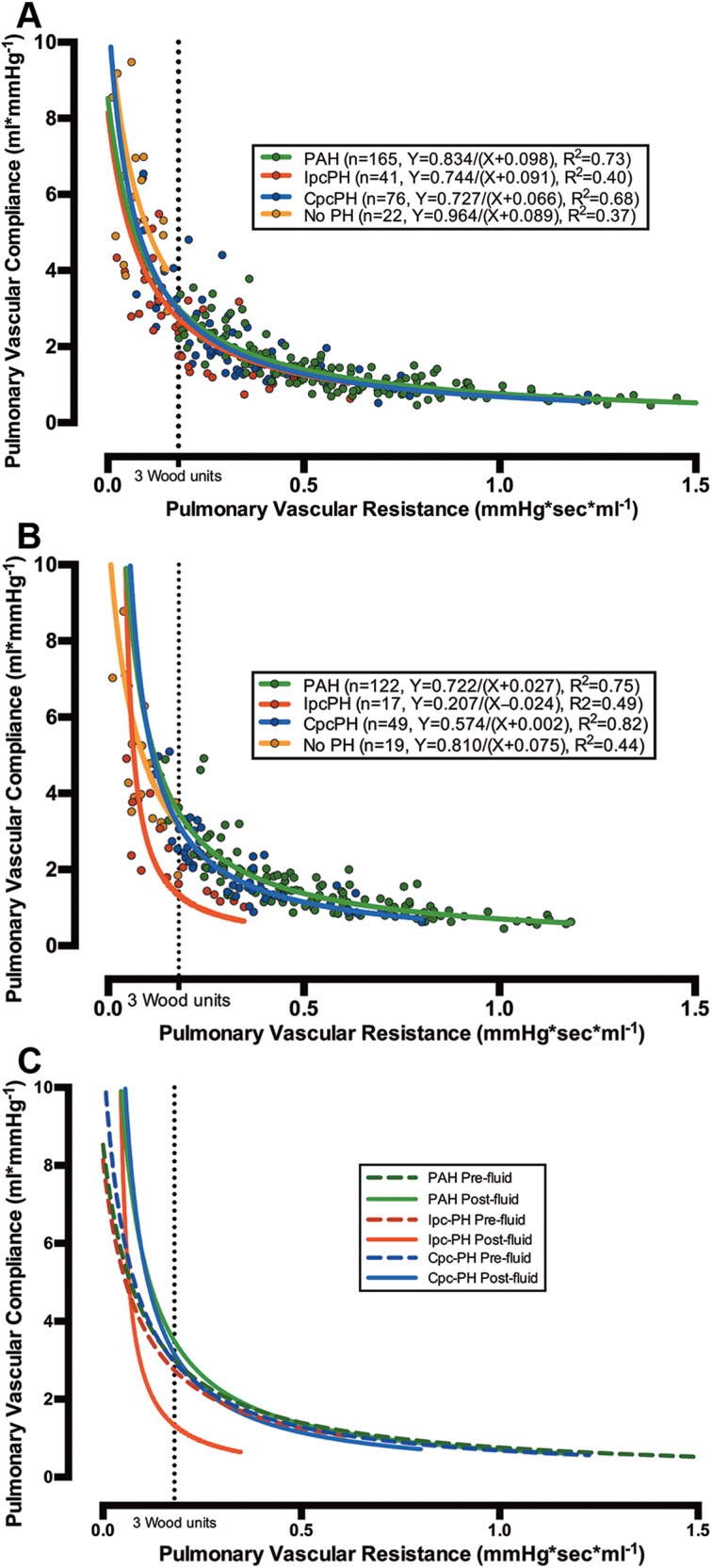
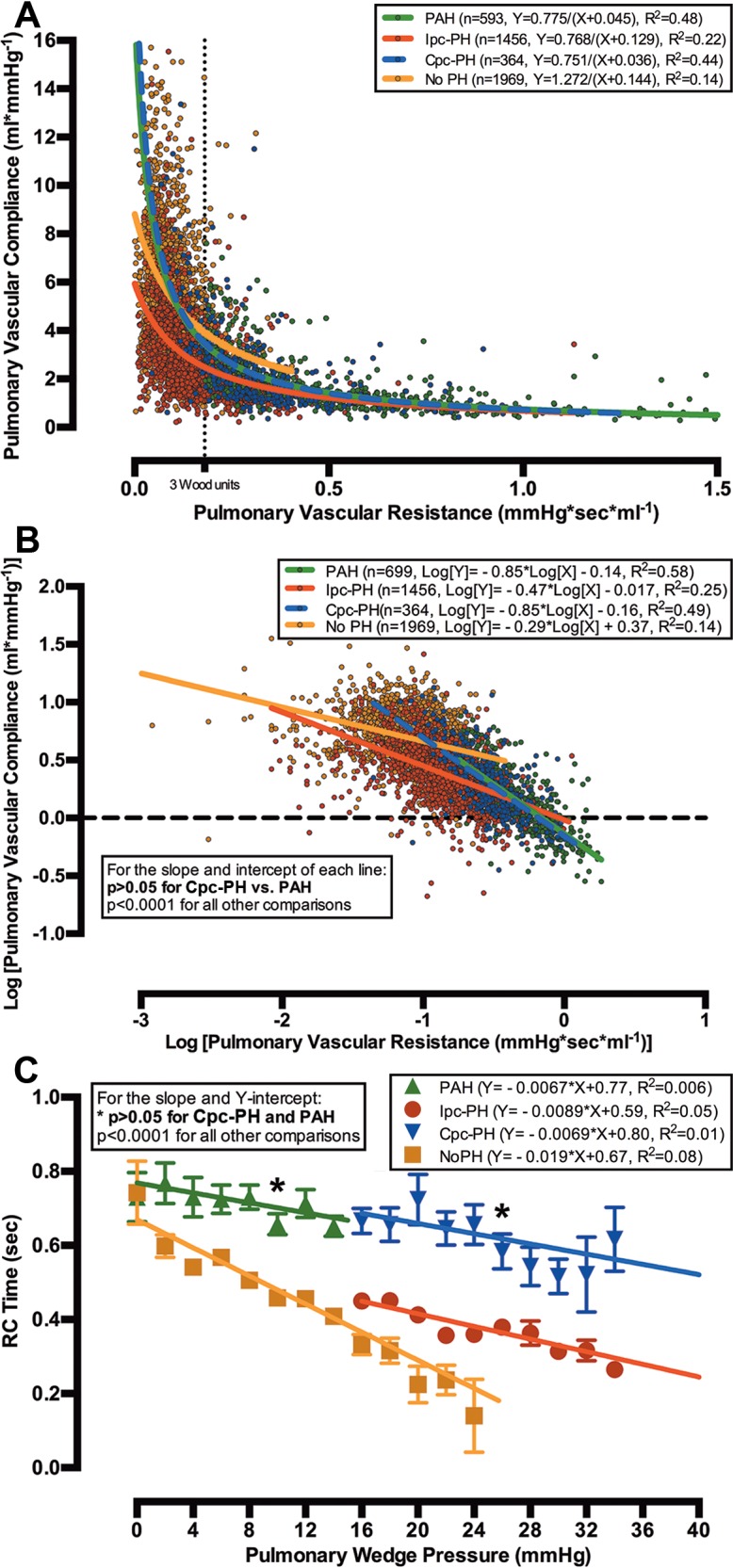
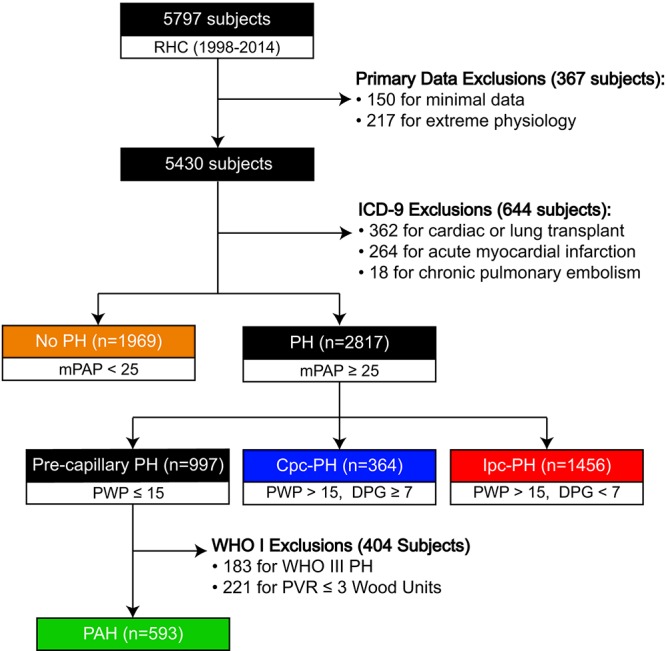
Although commonly encountered, patients with combined postcapillary and precapillary pulmonary hypertension (Cpc-PH) have poorly understood pulmonary vascular properties. The product of pulmonary vascular resistance and compliance, resistance-compliance (RC) time, is a measure of pulmonary vascular physiology. While RC time is lower in postcapillary PH than in precapillary PH, the RC time in Cpc-PH and the effect of pulmonary wedge pressure (PWP) on RC time are unknown. We tested the hypothesis that Cpc-PH has an RC time that resembles that in pulmonary arterial hypertension (PAH) more than that in isolated postcapillary PH (Ipc-PH). We analyzed the hemodynamics of 282 consecutive patients with PH referred for right heart catheterization (RHC) with a fluid challenge from 2004 to 2013 (cohort A) and 4,382 patients who underwent RHC between 1998 and 2014 for validation (cohort B). Baseline RC time in Cpc-PH was higher than that in Ipc-PH and lower than that in PAH in both cohorts (P < 0.001). In cohort A, RC time decreased after fluid challenge in patients with Ipc-PH but not in those with PAH or Cpc-PH (P < 0.001). In cohort B, the inverse relationship of pulmonary vascular compliance and resistance, as well as that of RC time and PWP, in Cpc-PH was similar to that in PAH and distinct from that in Ipc-PH. Our findings demonstrate that patients with Cpc-PH have pulmonary vascular physiology that resembles that of patients with PAH more than that of Ipc-PH patients. Further study is warranted to identify determinants of vascular remodeling and assess therapeutic response in this subset of PH.
Keywords: postcapillary; precapillary; pulmonary hypertension; pulmonary vascular compliance; pulmonary vascular resistance; resistance-compliance time.
Figures
References
-
- Fox BD, Shimony A, Langleben D, Hirsch A, Rudski L, Schlesinger R, Eisenberg MJ, et al. High prevalence of occult left heart disease in scleroderma-pulmonary hypertension. Eur Respir J 2013;42(4):1083–1091. - PubMed
-
- Andersen MJ, Olson TP, Melenovsky V, Kane GC, Borlaug BA. Differential hemodynamic effects of exercise and volume expansion in people with and without heart failure. Circ Heart Fail 2015;8(1):41–48. - PubMed
-
- Naeije R, Vachiéry JL, Yerly P, Vanderpool R. The transpulmonary pressure gradient for the diagnosis of pulmonary vascular disease. Eur Respir J 2013;41(1):217–223. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
