

Assessment of the physiologic contribution of right atrial function to total right heart function in patients with and without pulmonary arterial hypertension
- PMID: 27683609
- PMCID: PMC5019085
- DOI: 10.1086/687767
Assessment of the physiologic contribution of right atrial function to total right heart function in patients with and without pulmonary arterial hypertension
Abstract
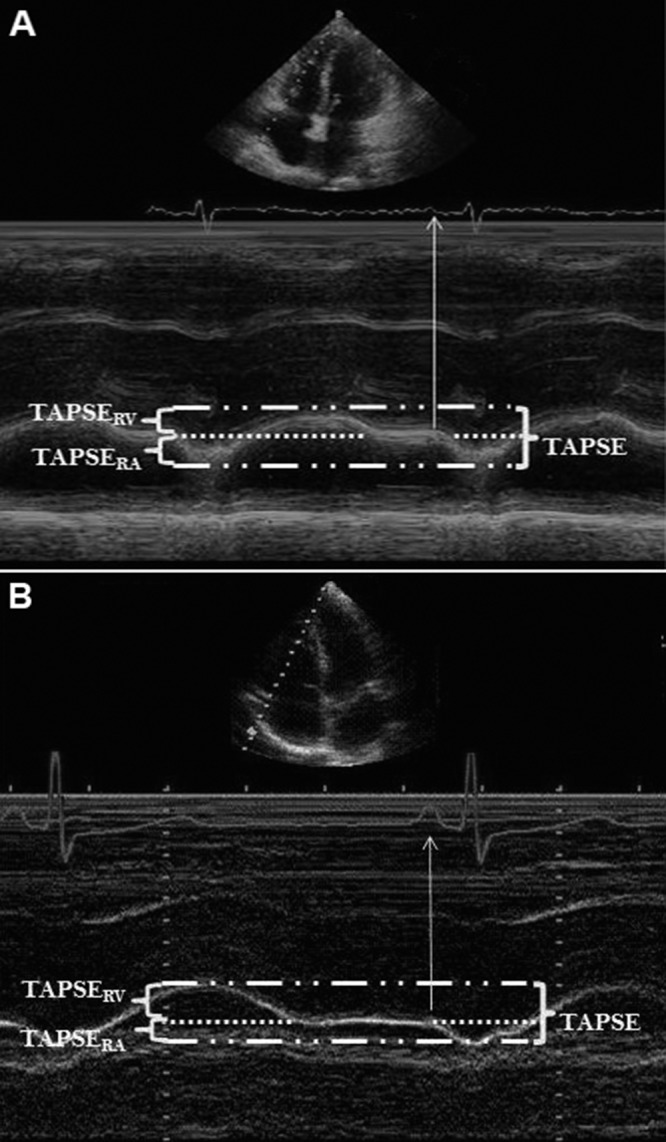
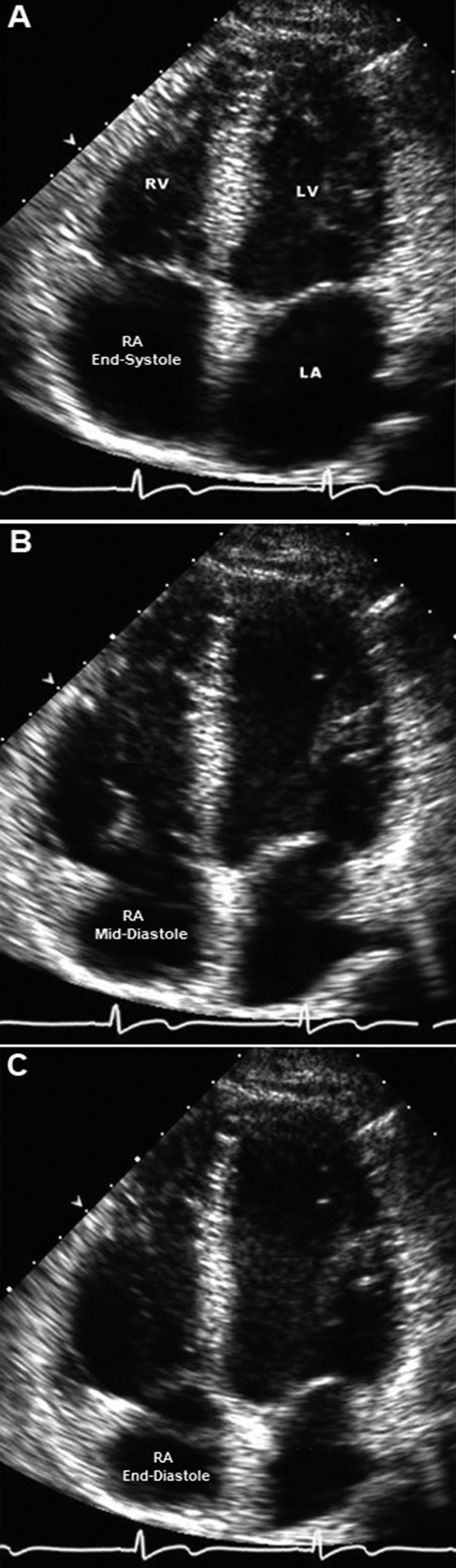
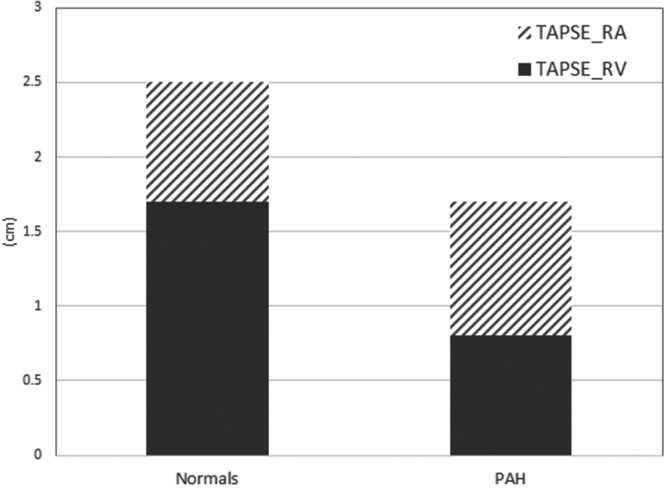
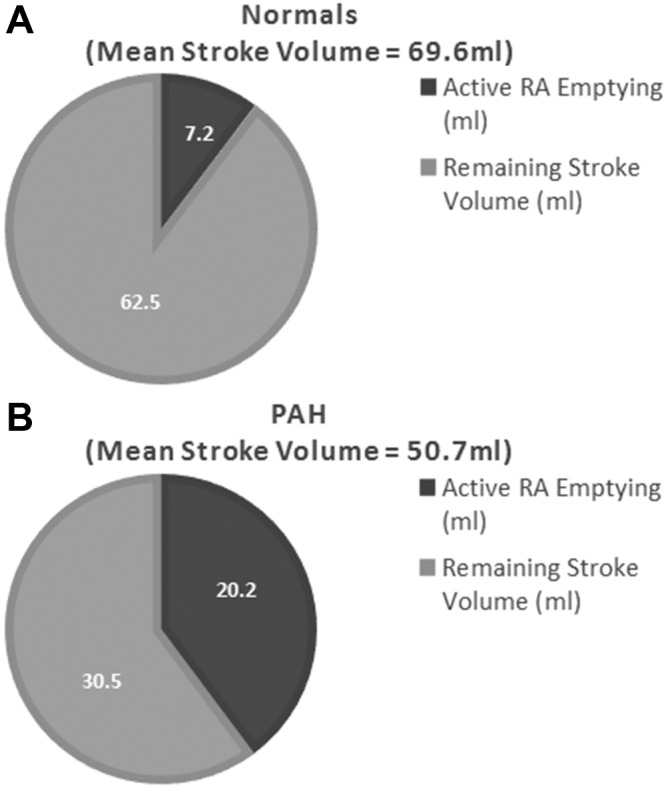
Total right heart function requires normal function of both the right ventricle and the right atrium. However, the degree to which right atrial (RA) function and right ventricular (RV) function each contribute to total right heart function has not been quantified. In this study, we aimed to quantify the contribution of RA function to total right heart function in a group of pulmonary arterial hypertension (PAH) patients compared to a cohort of normal controls without cardiovascular disease. The normal cohort comprised 35 subjects with normal clinical echocardiograms, while the PAH cohort included 37 patients, of whom 31 had echocardiograms before and after initiation of PAH-specific therapy. Total right heart function was measured via tricuspid annular plane excursion (TAPSE). TAPSE was broken down into two components, the excursion occurring during RA contraction (TAPSERA) and that occurring before RA contraction (TAPSERV). RA fractional area change (RA-FAC) was also compared between the two groups. In the PAH cohort, more than half of the total TAPSE occurred during atrial systole, compared to less than one-third in the normal cohort (51.0% vs. 32.1%; P < 0.0001). There was a significant correlation between RA-FAC and TAPSE in the PAH cohort but not in the normal cohort. TAPSE improved significantly in the posttreatment cohort (1.7 vs. 2.1 cm), but TAPSERA continued to account for about half of the total TAPSE after treatment. RA function accounts for a significantly greater proportion of total right heart function in patients with PAH than in normal subjects.
Keywords: echocardiography; right ventricular failure; tricuspid annular plane systolic excursion.
Figures
Similar articles
-
Maximal systolic excursion of the tricuspid annulus is independent of right atrial size and function in chronic pulmonary hypertension.Echocardiography. 2017 Jun;34(6):810-816. doi: 10.1111/echo.13531. Epub 2017 Apr 7. Echocardiography. 2017. PMID: 28386967 Free PMC article.
-
Longitudinal shortening accounts for the majority of right ventricular contraction and improves after pulmonary vasodilator therapy in normal subjects and patients with pulmonary arterial hypertension.Chest. 2011 Jul;140(1):27-33. doi: 10.1378/chest.10-1136. Epub 2010 Nov 24. Chest. 2011. PMID: 21106653
-
[Value of four-dimensional echocardiography combined with speckle tracking technique on the assessment of right heart function and prognosis in patients with pulmonary arterial hypertension].Zhonghua Xin Xue Guan Bing Za Zhi. 2018 Dec 24;46(12):965-971. doi: 10.3760/cma.j.issn.0253-3758.2018.12.007. Zhonghua Xin Xue Guan Bing Za Zhi. 2018. PMID: 30572401 Chinese.
-
Tricuspid annular displacement predicts survival in pulmonary hypertension.Am J Respir Crit Care Med. 2006 Nov 1;174(9):1034-41. doi: 10.1164/rccm.200604-547OC. Epub 2006 Aug 3. Am J Respir Crit Care Med. 2006. PMID: 16888289
-
Echocardiographic findings associated with mortality ortransplant in patients with pulmonary arterial hypertension:A systematic review and meta-analysis.Neth Heart J. 2016 Jun;24(6):374-389. doi: 10.1007/s12471-016-0845-3. Neth Heart J. 2016. PMID: 27189216 Free PMC article. Review.
Cited by
-
Arrhythmias in Patients with Pulmonary Hypertension and Right Ventricular Failure: Importance of Rhythm Control Strategies.J Clin Med. 2024 Mar 24;13(7):1866. doi: 10.3390/jcm13071866. J Clin Med. 2024. PMID: 38610631 Free PMC article. Review.
-
Simple electrocardiographic index for A4-wave amplitude of the VDD leadless pacemaker.Heart Rhythm O2. 2025 Jan 17;6(4):519-527. doi: 10.1016/j.hroo.2025.01.006. eCollection 2025 Apr. Heart Rhythm O2. 2025. PMID: 40321726 Free PMC article.
-
Right atrial function for the prediction of prognosis in connective tissue disease-associated pulmonary arterial hypertension: a study with two-dimensional speckle tracking.Int J Cardiovasc Imaging. 2019 Sep;35(9):1637-1649. doi: 10.1007/s10554-019-01613-w. Epub 2019 Apr 29. Int J Cardiovasc Imaging. 2019. PMID: 31037473
-
Maximal systolic excursion of the tricuspid annulus is independent of right atrial size and function in chronic pulmonary hypertension.Echocardiography. 2017 Jun;34(6):810-816. doi: 10.1111/echo.13531. Epub 2017 Apr 7. Echocardiography. 2017. PMID: 28386967 Free PMC article.
-
Left atrial to coronary sinus shunting in more advanced heart failure with preserved ejection fraction.ESC Heart Fail. 2025 Mar 16;12(4):2583-90. doi: 10.1002/ehf2.15270. Online ahead of print. ESC Heart Fail. 2025. PMID: 40090887 Free PMC article.
References
-
- McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, Mathier MA, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol 2009;53(17):1573–1619. - PubMed
-
- Galiè N, Manes A, Palazzini M, Negro L, Romanazzi S, Branzi A. Pharmacological impact on right ventricular remodelling in pulmonary arterial hypertension. Eur Heart J Suppl 2007;9(H):H68–H74.
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, et al. Survival in patients with primary pulmonary hypertension: results from a national prospective registry. Ann Intern Med 1991;115(5):343–349. - PubMed
-
- Mehra MR, Park MH, Landzberg MJ, Lala A, Waxman AB. Right heart failure: toward a common language. J Heart Lung Transplant 2014;33(2):123–126. - PubMed
-
- Goldstein JA, Harada A, Yagi Y, Barzilai B, Cox JL. Hemodynamic importance of systolic ventricular interaction, augmented right atrial contractility and atrioventricular synchrony in acute right ventricular dysfunction. J Am Coll Cardiol 1990;16(1):181–189. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
