

Percutaneous thoracolumbar decompression combined with percutaneous pedicle screw fixation and fusion: a method for treating spinal degenerative pain in a biplane angiography suite with the avoidance of general anesthesia
- PMID: 27683708
- PMCID: PMC5039853
- DOI: 10.21037/jss.2016.06.03
Percutaneous thoracolumbar decompression combined with percutaneous pedicle screw fixation and fusion: a method for treating spinal degenerative pain in a biplane angiography suite with the avoidance of general anesthesia
Abstract
Background: Spondylytic degeneration of the axial lumbar spine is a major cause of pain and disability. Recent advances in spinal surgical instrumentation, including percutaneous access and fusion techniques, have made possible the performance of instrumented fusion through small incisions. By blending strategies of interventional pain management, neuroradiology, and conventional spine surgery, it is now feasible to treat spinal axial pain using permanent fixation techniques and local anesthesia in the setting of a fluoroscopy suite using mild sedation and local anesthesia.
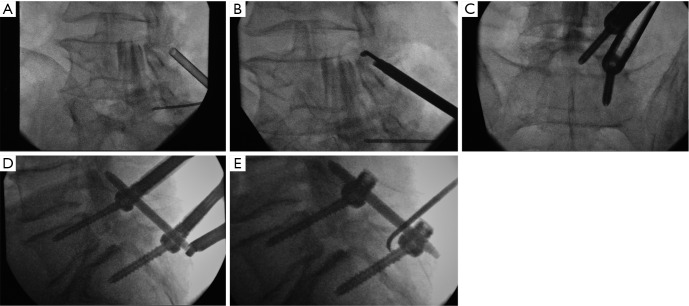
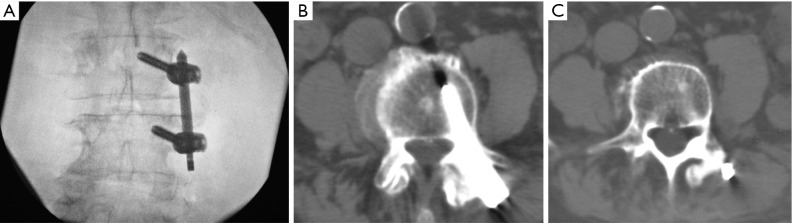
Methods: The author presents a series of percutaneous thoracolumbar fusion procedures performed in a biplane neuroangiographic suite and without general anesthesia for the treatment of spondylytic pain. All procedures utilized pedicle screw fixation, harvesting of local bone autograft, and application of bone fusion material.
Results: In this series of 13 patients, a statistically significant reduction of pain was seen at both the 2-week post-operative timepoint, as well as at the time of longest follow-up (mean 40 weeks).
Discussion: The advanced and rapid imaging capabilities afforded by a neuroangiographic suite can be safely combined with percutaneous fusion techniques so as to allow for fusion therapies to be applied to patients where the avoidance of general anesthesia is desirable.
Keywords: Spondylosis; biplane suite; fusion; pedicle screw; sedation.
Conflict of interest statement
Dr. Chopko is a consultant as well as a member of the Scientific Advisory Board for Vertos Medical, and has received compensation in the form of consulting fees and stock option grants. During the time of data collection, Dr. Chopko was a consultant for Bacterin International Holdings, where he received compensation in the form of consulting fees, and was also a member of the Scientific Advisory Board.
Figures

References
-
- Kim CW, Siemionow K, Anderson DG, et al. The current state of minimally invasive spine surgery. J Bone Joint Surg Am 2011;93:582-96. - PubMed
-
- Dong J, Rong L, Feng F, et al. Unilateral pedicle screw fixation through a tubular retractor via the Wiltse approach compared with conventional bilateral pedicle screw fixation for single-segment degenerative lumbar instability: a prospective randomized study. J Neurosurg Spine 2014;20:53-9. 10.3171/2013.9.SPINE1392 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources