

Randomized Controlled Trials to Define Viral Load Thresholds for Cytomegalovirus Pre-Emptive Therapy
- PMID: 27684379
- PMCID: PMC5042415
- DOI: 10.1371/journal.pone.0163722
Randomized Controlled Trials to Define Viral Load Thresholds for Cytomegalovirus Pre-Emptive Therapy
Erratum in
-
Correction: Randomized Controlled Trials to Define Viral Load Thresholds for Cytomegalovirus Pre-Emptive Therapy.PLoS One. 2017 Sep 19;12(9):e0185298. doi: 10.1371/journal.pone.0185298. eCollection 2017. PLoS One. 2017. PMID: 28926631 Free PMC article.
Abstract
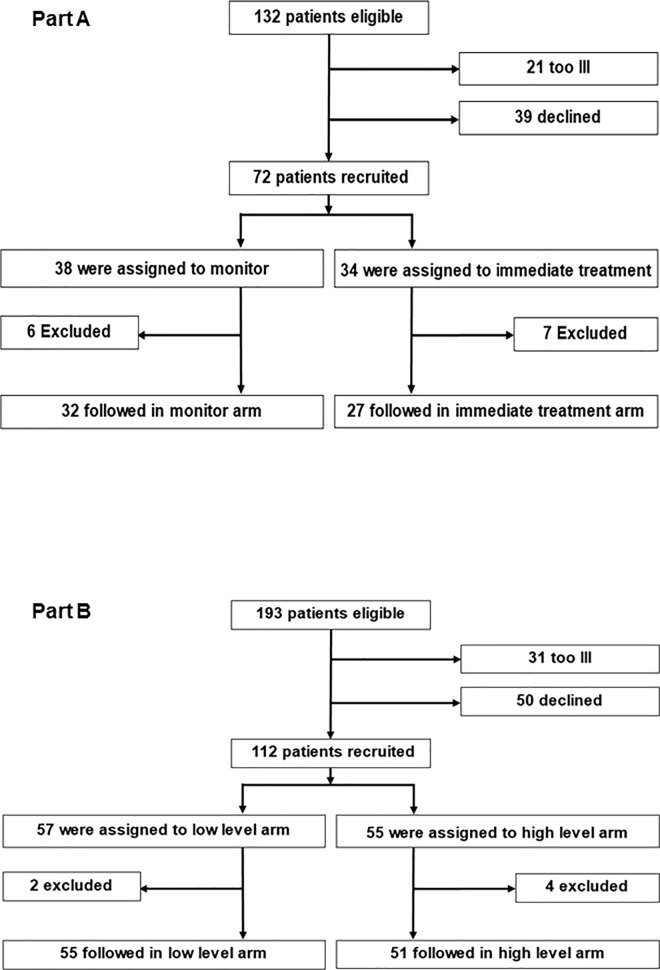
Background: To help decide when to start and when to stop pre-emptive therapy for cytomegalovirus infection, we conducted two open-label randomized controlled trials in renal, liver and bone marrow transplant recipients in a single centre where pre-emptive therapy is indicated if viraemia exceeds 3000 genomes/ml (2520 IU/ml) of whole blood.
Methods: Patients with two consecutive viraemia episodes each below 3000 genomes/ml were randomized to continue monitoring or to immediate treatment (Part A). A separate group of patients with viral load greater than 3000 genomes/ml was randomized to stop pre-emptive therapy when two consecutive levels less than 200 genomes/ml (168 IU/ml) or less than 3000 genomes/ml were obtained (Part B). For both parts, the primary endpoint was the occurrence of a separate episode of viraemia requiring treatment because it was greater than 3000 genomes/ml.
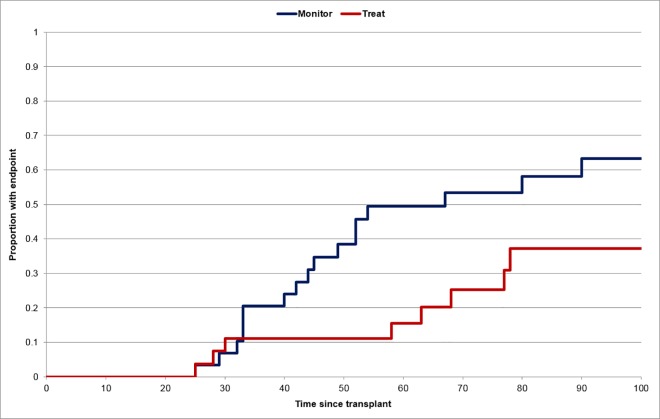
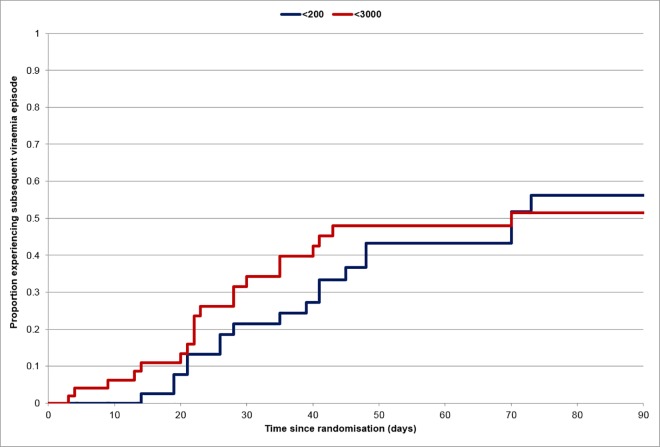
Results: In Part A, the primary endpoint was not significantly different between the two arms; 18/32 (56%) in the monitor arm had viraemia greater than 3000 genomes/ml compared to 10/27 (37%) in the immediate treatment arm (p = 0.193). However, the time to developing an episode of viraemia greater than 3000 genomes/ml was significantly delayed among those randomized to immediate treatment (p = 0.022). In Part B, the primary endpoint was not significantly different between the two arms; 19/55 (35%) in the less than 200 genomes/ml arm subsequently had viraemia greater than 3000 genomes/ml compared to 23/51 (45%) among those randomized to stop treatment in the less than 3000 genomes/ml arm (p = 0.322). However, the duration of antiviral treatment was significantly shorter (p = 0.0012) in those randomized to stop treatment when viraemia was less than 3000 genomes/ml.
Discussion: The results illustrate that patients have continuing risks for CMV infection with limited time available for intervention. We see no need to alter current rules for stopping or starting pre-emptive therapy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Reusser P, Einsele H, Lee J, Volin L, Rovira M, Engelhard D, et al. Randomized multicenter trial of foscarnet versus ganciclovir for pre-emptive therapy of cytomegalovirus infection after allogeneic stem cell transplantation. Blood 2002; 99: 1159–1164. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
