

Prospective economic evaluation alongside the non-invasive ventilation trial
- PMID: 27684419
- PMCID: PMC6955038
- DOI: 10.1038/jp.2016.159
Prospective economic evaluation alongside the non-invasive ventilation trial
Abstract
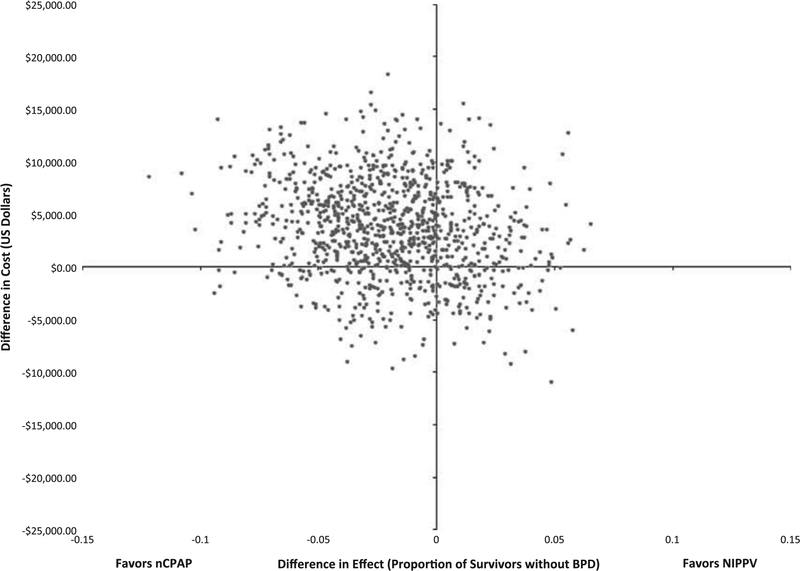
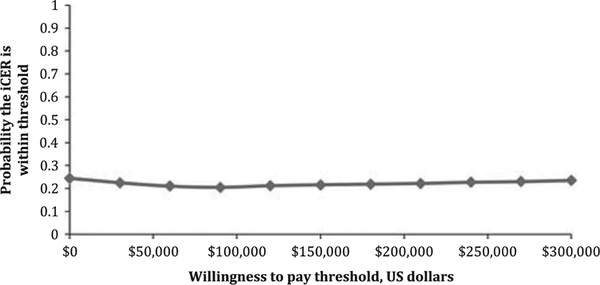
Objective: To determine the cost-effectiveness of nasal continuous positive pressure (nCPAP) compared with nasal intermittent positive pressure ventilation (NIPPV) in the context of the reported randomized clinical trial.
Study design: Using patient-level data from the clinical trial, we undertook a prospectively planned economic evaluation. We measured costs, from a third-party payer perspective in all patients, and from a societal perspective in a subgroup with a time horizon through the earlier of discharge, death or 44 weeks post-menstrual age.
Results: From the third-party payer perspective, the mean cost of hospitalization per infant was statistically similar, $143 745 in the NIPPV group compared to $140 403 in the nCPAP group. Cost-effectiveness evaluation revealed a 61% probability that NIPPV is more expensive and less effective than nCPAP. Similar results were found in subgroup analysis from a societal perspective.
Conclusion: In addition to being clinically equivalent, economic evaluation confirms that NIPPV, as employed in this trial, is also not economically favorable.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declare no conflict of interest.
Figures
References
-
- Horbar JD, Carpenter JH, Badger GJ, Kenny MJ, Soll RF, Morrow KA et al. Mortality and neonatal morbidity among infants 501 to 1500 grams from 2000 to 2009. Pediatrics 2012; 129(6): 1019–1026. - PubMed
-
- Fischer HS, Buhrer C. Avoiding endotracheal ventilation to prevent bronchopulmonary dysplasia: a meta-analysis. Pediatrics 2013; 132(5): e1351–e1360. - PubMed
-
- Latini G, De Felice HC, Giannuzzi R, Del Vecchio A. Survival rate and prevalence of bronchopulmonary dysplasia in extremely low birth weight infants. Early Hum Dev 2013; 89(Suppl 1): S69–S73. - PubMed
-
- Dunn MS, Kaempf J, de Klerk A, de Klerk R, Reilly M, Howard D et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics 2011; 128(5): e1069–e1076. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
