

On the use of a convolution-superposition algorithm for plan checking in lung stereotactic body radiation therapy
- PMID: 27685114
- PMCID: PMC5874108
- DOI: 10.1120/jacmp.v17i5.6186
On the use of a convolution-superposition algorithm for plan checking in lung stereotactic body radiation therapy
Abstract
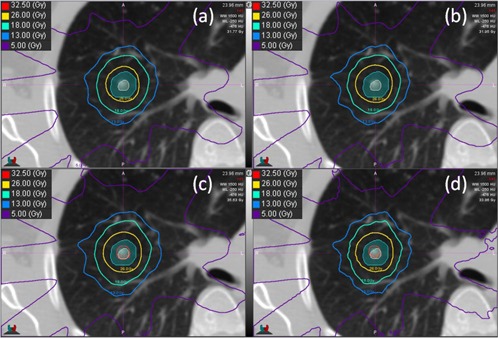
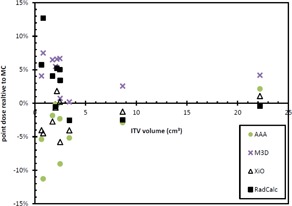
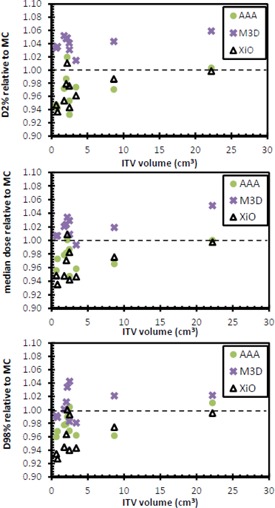
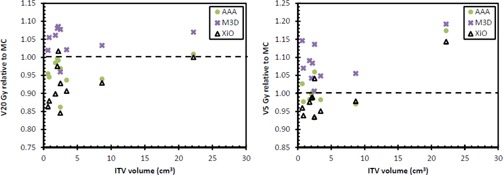
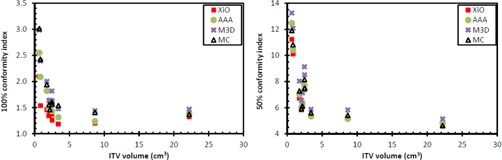
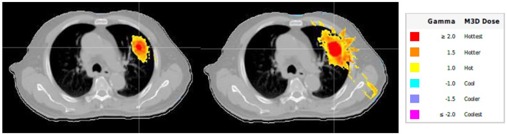
Stereotactic body radiation therapy (SBRT) aims to deliver a highly conformal ablative dose to a small target. Dosimetric verification of SBRT for lung tumors presents a challenge due to heterogeneities, moving targets, and small fields. Recent software (M3D) designed for dosimetric verification of lung SBRT treatment plans using an advanced convolution-superposition algorithm was evaluated. Ten lung SBRT patients covering a range of tumor volumes were selected. 3D CRT plans were created using the XiO treatment planning system (TPS) with the superposition algorithm. Dose was recalculated in the Eclipse TPS using the AAA algorithm, M3D verification software using the collapsed-cone-convolution algorithm, and in-house Monte Carlo (MC). Target point doses were calculated with RadCalc software. Near-maximum, median, and near-minimum target doses, conformity indices, and lung doses were compared with MC as the reference calculation. M3D 3D gamma passing rates were compared with the XiO and Eclipse. Wilcoxon signed-rank test was used to compare each calculation method with XiO with a threshold of significance of p < 0.05. M3D and RadCalc point dose calculations were greater than MC by up to 7.7% and 13.1%, respectively, with M3D being statistically significant (s.s.). AAA and XiO calculated point doses were less than MC by 11.3% and 5.2%, respectively (AAA s.s.). Median and near-minimum and near-maximum target doses were less than MC when calculated with AAA and XiO (all s.s.). Near-maximum and median target doses were higher with M3D compared with MC (s.s.), but there was no difference in near-minimum M3D doses compared with MC. M3D-calculated ipsilateral lung V20 Gy and V5 Gy were greater than that calculated with MC (s.s.); AAA- and XiO-calculated V20 Gy was lower than that calculated with MC, but not statistically different to MC for V5 Gy. Nine of the 10 plans achieved M3D gamma passing rates greater than 95% and 80%for 5%/1 mm and 3%/1 mm criteria, respectively. M3D typically calculated a higher target and lung dose than MC for lung SBRT plans. The results show a range of calculated doses with different algorithms and suggest that M3D is in closer agree-ment with Monte Carlo, thus discrepancies between the TPS and M3D software will be observed for lung SBRT plans. M3D provides a useful supplement to verification of lung SBRT plans by direct measurement, which typically excludes patient specific heterogeneities.
© 2016 The Authors.
Figures
Similar articles
-
Assessment of Monte Carlo algorithm for compliance with RTOG 0915 dosimetric criteria in peripheral lung cancer patients treated with stereotactic body radiotherapy.J Appl Clin Med Phys. 2016 May 8;17(3):277-293. doi: 10.1120/jacmp.v17i3.6077. J Appl Clin Med Phys. 2016. PMID: 27167284 Free PMC article.
-
Dosimetric verification using monte carlo calculations for tissue heterogeneity-corrected conformal treatment plans following RTOG 0813 dosimetric criteria for lung cancer stereotactic body radiotherapy.Int J Radiat Oncol Biol Phys. 2012 Oct 1;84(2):508-13. doi: 10.1016/j.ijrobp.2011.12.005. Epub 2012 Feb 24. Int J Radiat Oncol Biol Phys. 2012. PMID: 22365630 Free PMC article.
-
Performance of dose calculation algorithms from three generations in lung SBRT: comparison with full Monte Carlo-based dose distributions.J Appl Clin Med Phys. 2014 Mar 6;15(2):4662. doi: 10.1120/jacmp.v15i2.4662. J Appl Clin Med Phys. 2014. PMID: 24710454 Free PMC article.
-
Influence of the jaw tracking technique on the dose calculation accuracy of small field VMAT plans.J Appl Clin Med Phys. 2017 Jan;18(1):186-195. doi: 10.1002/acm2.12029. Epub 2017 Jan 3. J Appl Clin Med Phys. 2017. PMID: 28291941 Free PMC article. Review.
-
[Investigating the clinical applicability of EBT2 self-developing films].Magy Onkol. 2016 Nov 29;60(4):299-304. Epub 2016 May 25. Magy Onkol. 2016. PMID: 27898748 Review. Hungarian.
Cited by
-
The Effect of Algorithms on Dose Distribution in Inhomogeneous Phantom: Monaco Treatment Planning System versus Monte Carlo Simulation.J Med Phys. 2021 Apr-Jun;46(2):111-115. doi: 10.4103/jmp.JMP_21_21. Epub 2021 Aug 7. J Med Phys. 2021. PMID: 34566291 Free PMC article.
-
Technical note: A modified gamma evaluation method for dose distribution comparisons.J Appl Clin Med Phys. 2019 Jul;20(7):193-200. doi: 10.1002/acm2.12606. J Appl Clin Med Phys. 2019. PMID: 31282112 Free PMC article.
References
-
- Siva S, MacManus M, Ball D. Stereotactic radiotherapy for pulmonary oligometastases: a systematic review. J Thorac Oncol. 2010;5(7):1091–99. - PubMed
-
- Wulf J, Haedinger U, Oppitz U, Thiele W, Mueller G, Flentje M. Stereotactic radiotherapy for primary lung cancer and pulmonary metastases: a noninvasive treatment approach in medically inoperable patients. Int J Radiat Oncol Biol Phys. 2004;60(1):186–96. - PubMed
-
- Benedict SH, Yenice KM, Followill D, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys. 2010;37(8):4078–101. - PubMed
-
- Knöös T, Wieslander E, Cozzi L, et al. Comparison of dose calculation algorithms for treatment planning in external photon beam therapy for clinical situations. Phys Med Biol. 2006;51(22):5785–807. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
