

Flow Conditions in the Intracranial Aneurysm Lumen Are Associated with Inflammation and Degenerative Changes of the Aneurysm Wall
- PMID: 27686488
- PMCID: PMC5233582
- DOI: 10.3174/ajnr.A4951
Flow Conditions in the Intracranial Aneurysm Lumen Are Associated with Inflammation and Degenerative Changes of the Aneurysm Wall
Abstract
Background and purpose: Saccular intracranial aneurysm is a common disease that may cause devastating intracranial hemorrhage. Hemodynamics, wall remodeling, and wall inflammation have been associated with saccular intracranial aneurysm rupture. We investigated how saccular intracranial aneurysm hemodynamics is associated with wall remodeling and inflammation of the saccular intracranial aneurysm wall.
Materials and methods: Tissue samples resected during a saccular intracranial aneurysm operation (11 unruptured, 9 ruptured) were studied with histology and immunohistochemistry. Patient-specific computational models of hemodynamics were created from preoperative CT angiographies.
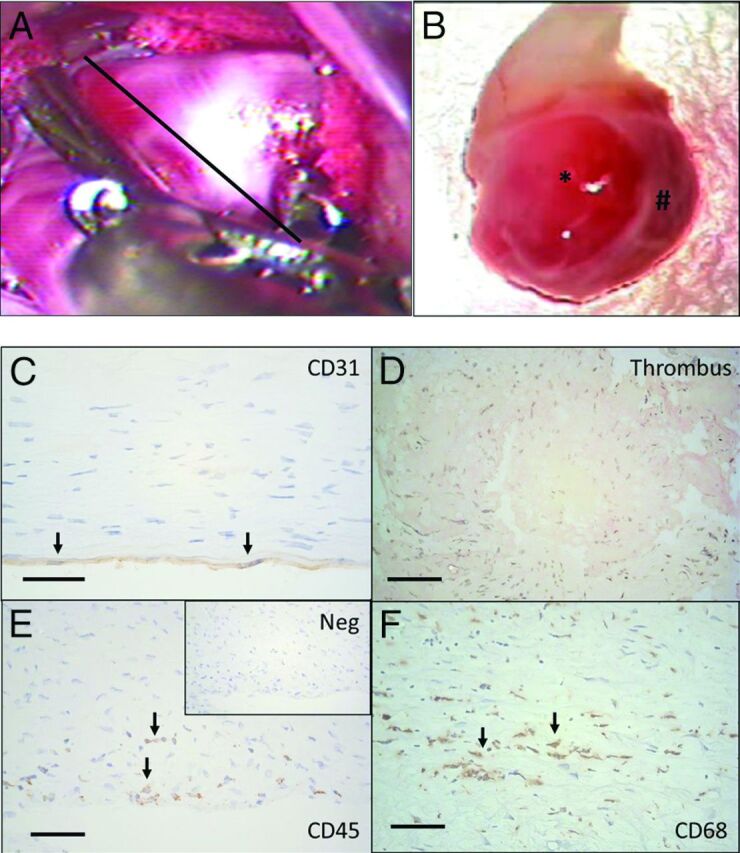
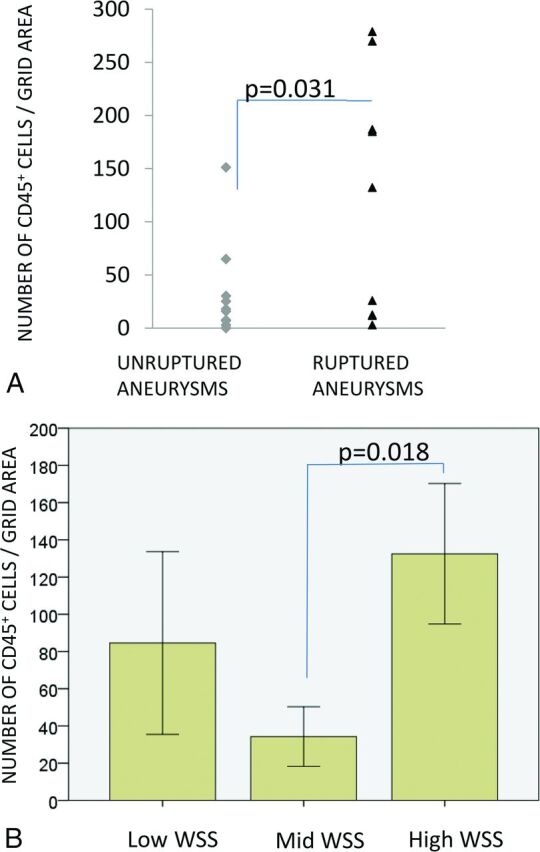
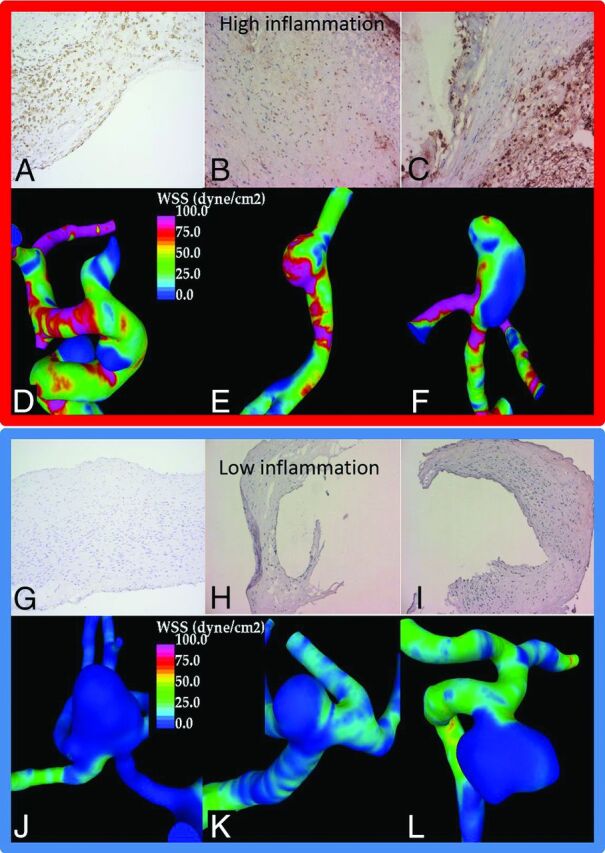
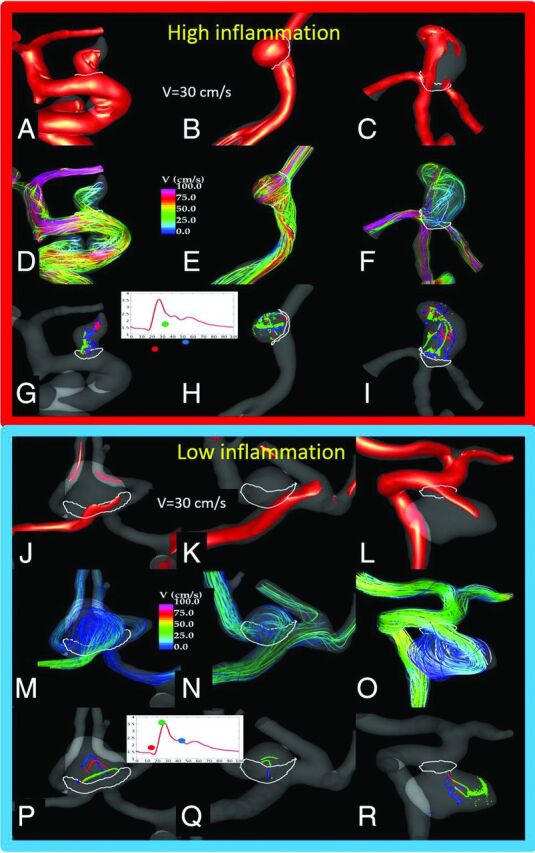
Results: More stable and less complex flows were associated with thick, hyperplastic saccular intracranial aneurysm walls, while slower flows with more diffuse inflow were associated with degenerated and decellularized saccular intracranial aneurysm walls. Wall degeneration (P = .041) and rupture were associated with increased inflammation (CD45+, P = .031). High wall shear stress (P = .018), higher vorticity (P = .046), higher viscous dissipation (P = .046), and high shear rate (P = .046) were associated with increased inflammation. Inflammation was also associated with lack of an intact endothelium (P = .034) and the presence of organized luminal thrombosis (P = .018), though overall organized thrombosis was associated with low minimum wall shear stress (P = .034) and not with the flow conditions associated with inflammation.
Conclusions: Flow conditions in the saccular intracranial aneurysm are associated with wall remodeling. Inflammation, which is associated with degenerative wall remodeling and rupture, is related to high flow activity, including elevated wall shear stress. Endothelial injury may be a mechanism by which flow induces inflammation in the saccular intracranial aneurysm wall. Hemodynamic simulations might prove useful in identifying saccular intracranial aneurysms at risk of developing inflammation, a potential biomarker for rupture.
© 2017 by American Journal of Neuroradiology.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous