

Integrating molecular markers into the World Health Organization classification of CNS tumors: a survey of the neuro-oncology community
- PMID: 27688263
- PMCID: PMC5464323
- DOI: 10.1093/neuonc/now181
Integrating molecular markers into the World Health Organization classification of CNS tumors: a survey of the neuro-oncology community
Abstract
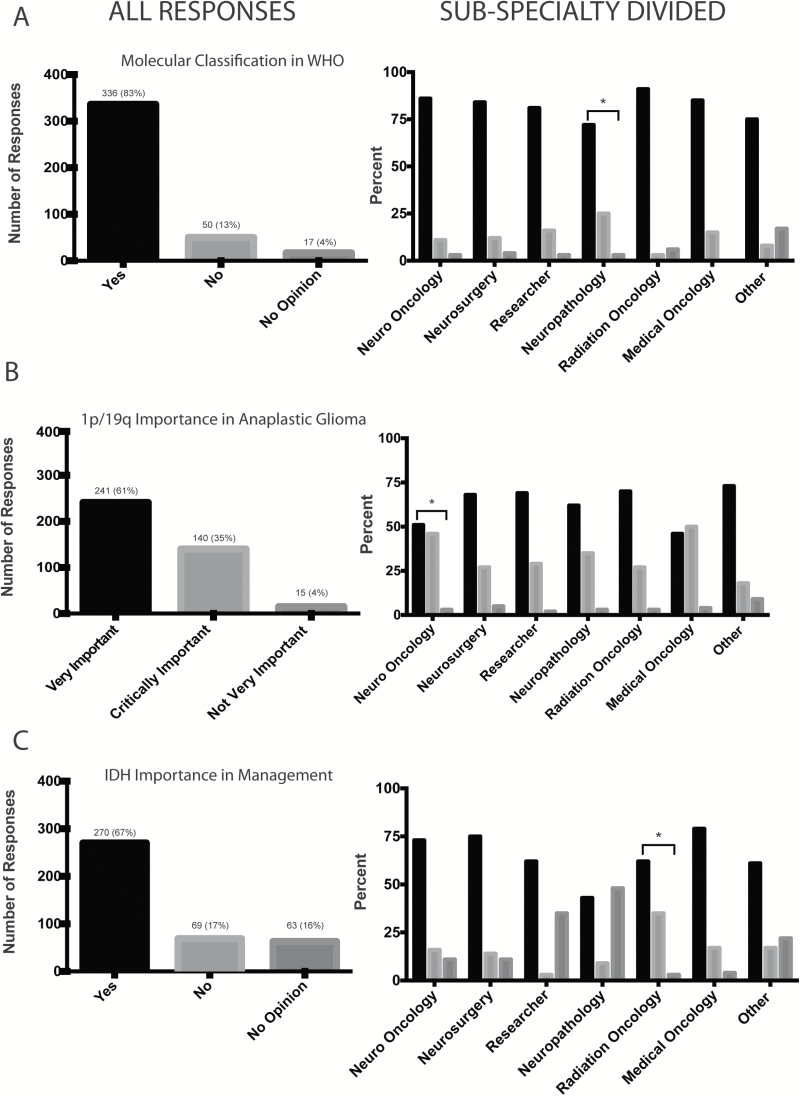
Background: Molecular markers provide important biological and clinical information related to the classification of brain tumors, and the integration of relevant molecular parameters into brain tumor classification systems has been a widely discussed topic in neuro-oncology over the past decade. With recent advances in the development of clinically relevant molecular signatures and the 2016 World Health Organization (WHO) update, the views of the neuro-oncology community on such changes would be informative for implementing this process.
Methods: A survey with 8 questions regarding molecular markers in tumor classification was sent to an email list of Society for Neuro-Oncology members and attendees of prior meetings (n=5065). There were 403 respondents. Analysis was performed using whole group response, based on self-reported subspecialty.
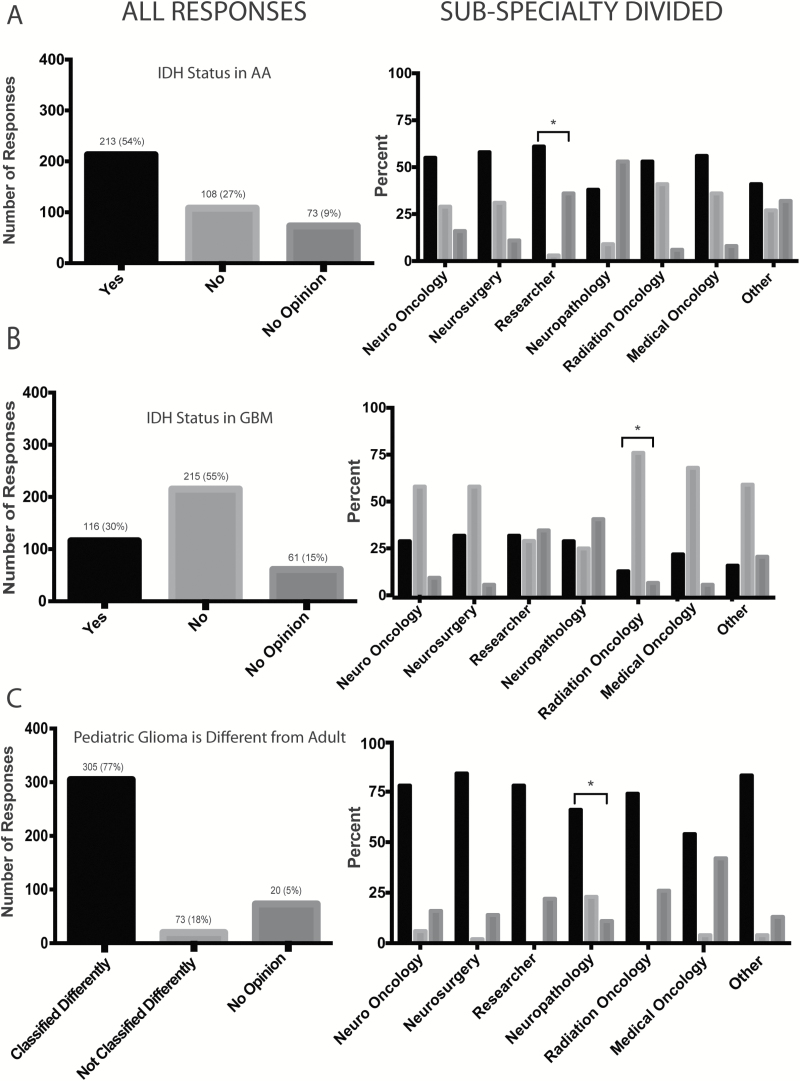
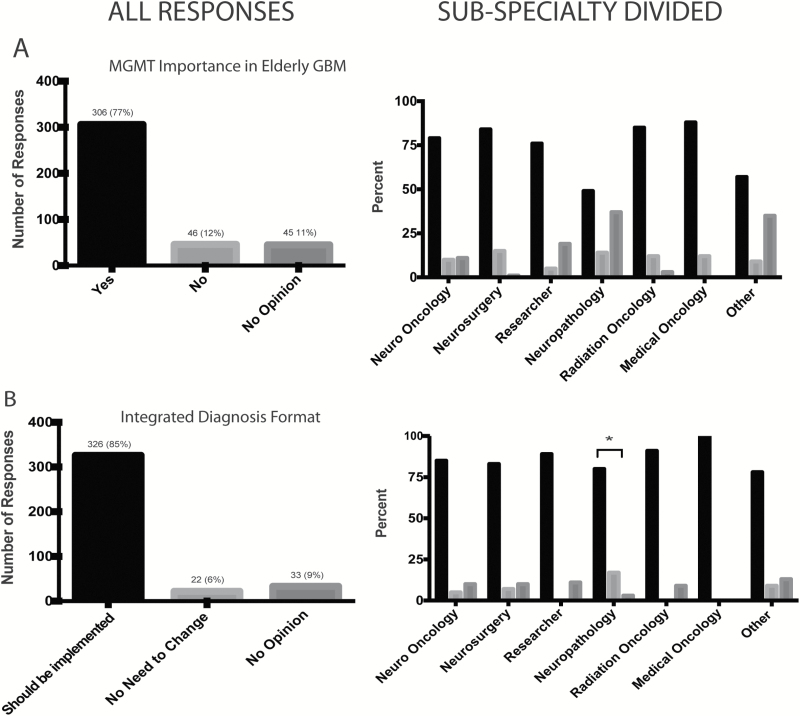
Results: The survey results show overall strong support for incorporating molecular knowledge into the classification and clinical management of brain tumors. Across all 7 subspecialty groups, ≥70% of respondents agreed to this integration. Interestingly, some variability is seen among subspecialties, notably with lowest support from neuropathologists, which may reflect their roles in implementing such diagnostic technologies.
Conclusion: Based on a survey provided to the neuro-oncology community, we report strong support for the integration of molecular markers into the WHO classification of brain tumors, as well as for using an integrated "layered" diagnostic format. While membership from each specialty showed support, there was variation by specialty in enthusiasm regarding proposed changes. The initial results of this survey influenced the deliberations underlying the 2016 WHO classification of tumors of the central nervous system.
Keywords: classification; molecular markers; pathology.
© The Author(s) 2017. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
References
-
- Louis DN OH, Wiestler OD, Cavenee WK. World Health Organization Histological Classification of Tumours of the Central Nervous System. Lyon: International Agency for Research on Cancer; 2007.
-
- Wiestler B, Capper D, Sill M, et al. Integrated DNA methylation and copy-number profiling identify three clinically and biologically relevant groups of anaplastic glioma. Acta Neuropathol. 2014;128(4):561–571. - PubMed
-
- Labussiere M, Boisselier B, Mokhtari K, et al. Combined analysis of TERT, EGFR, and IDH status defines distinct prognostic glioblastoma classes. Neurology. 2014;83(13):1200–1206. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
