

Fluorescence-guided surgery of a highly-metastatic variant of human triple-negative breast cancer targeted with a cancer-specific GFP adenovirus prevents recurrence
- PMID: 27689331
- PMCID: PMC5342766
- DOI: 10.18632/oncotarget.12314
Fluorescence-guided surgery of a highly-metastatic variant of human triple-negative breast cancer targeted with a cancer-specific GFP adenovirus prevents recurrence
Abstract
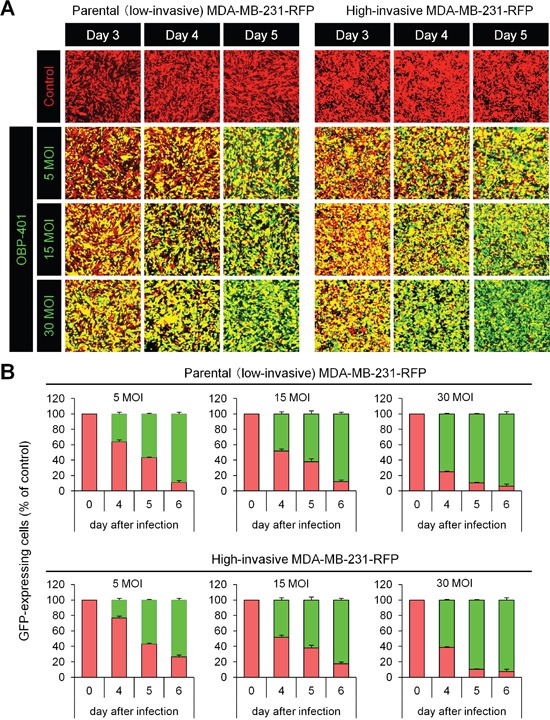
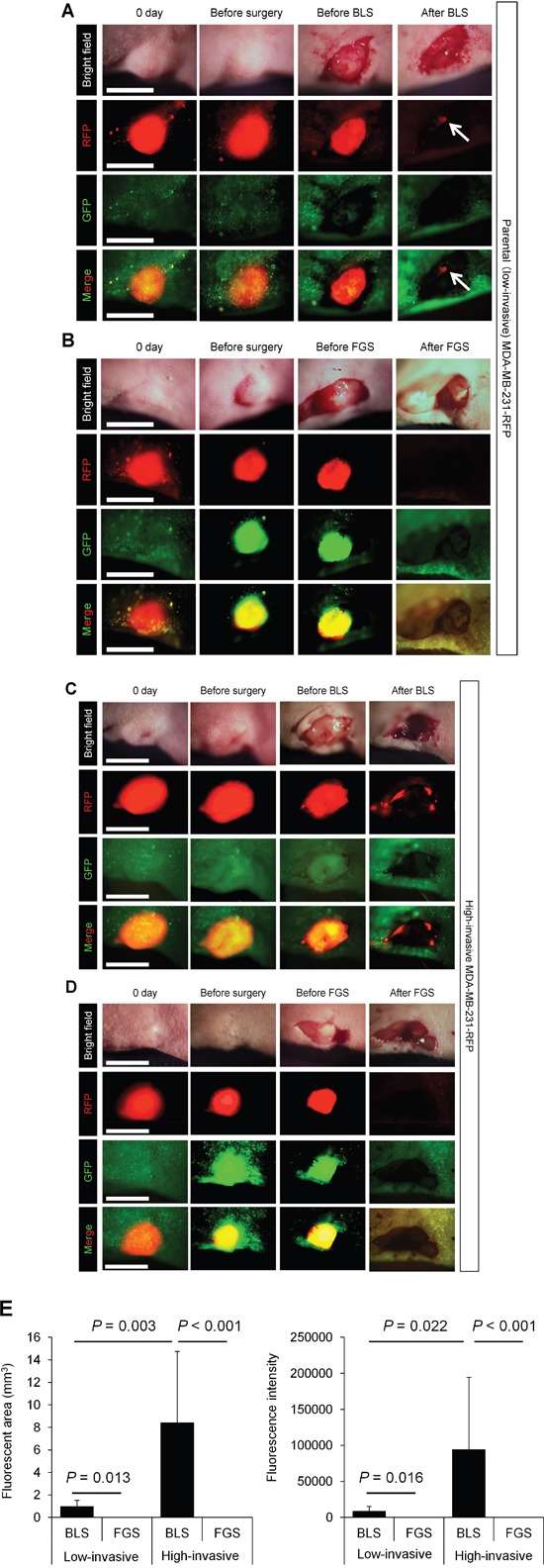
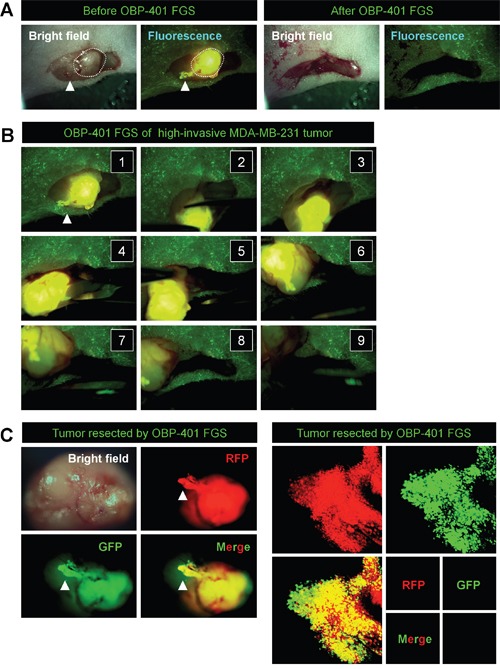
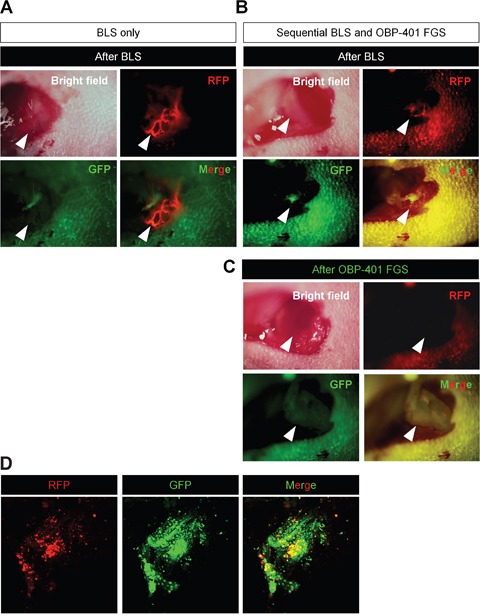
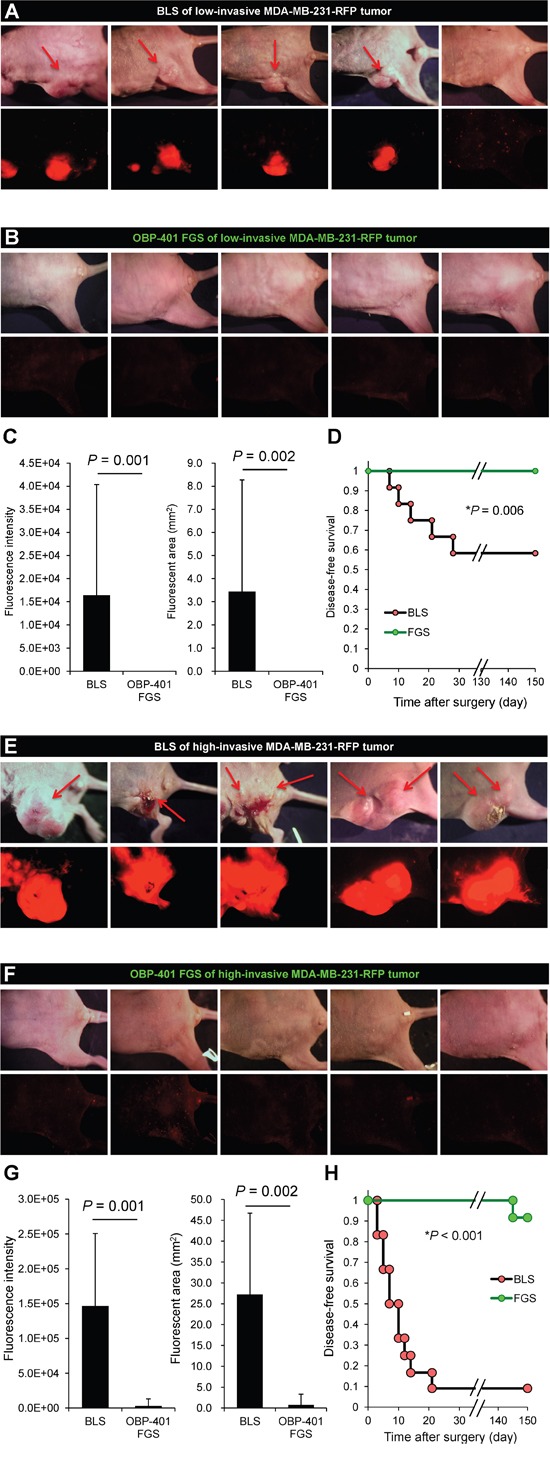
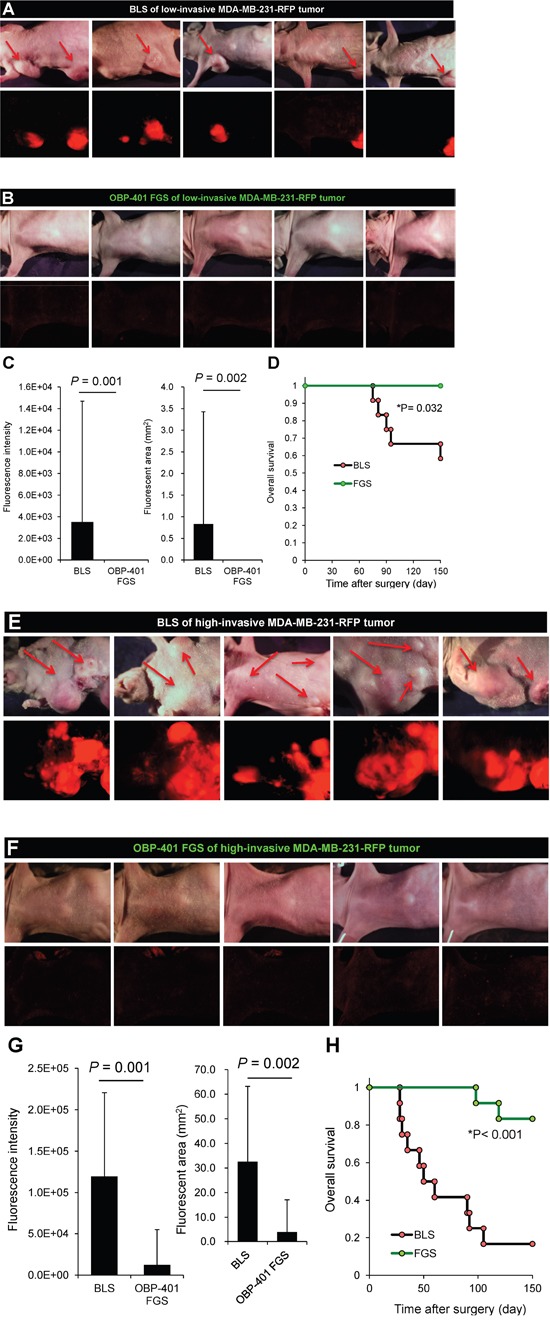
We have previously developed a genetically-engineered GFP-expressing telomerase-dependent adenovirus, OBP-401, which can selectively illuminate cancer cells. In the present report, we demonstrate that targeting a triple-negative high-invasive human breast cancer, orthotopically-growing in nude mice, with OBP-401 enables curative fluorescence-guided surgery (FGS). OBP-401 enabled complete resection and prevented local recurrence and greatly inhibited lymph-node metastasis due to the ability of the virus to selectively label and subsequently kill cancer cells. In contrast, residual breast cancer cells become more aggressive after bright (white)-light surgery (BLS). OBP-401-based FGS also improved the overall survival compared with conventional BLS. Thus, metastasis from a highly-aggressive triple-negative breast cancer can be prevented by FGS in a clinically-relevant mouse model.
Keywords: GFP/RFP; adenovirus; fluorescence-guided surgery (FGS); survival; telomerase dependent.
Conflict of interest statement
Y. Urata is a CEO of Oncolys BioPharma Inc. (the manufacturer of OBP-401). H. Tazawa and T. Fujiwara are consultants of Oncolys BioPharma Inc.
Figures
References
-
- Bouvet M, Hoffman RM. Glowing tumors make for better detection and resection. Sci Transl Med. 2011;3:110sf10. - PubMed
-
- Yano S, Miwa S, Kishimoto H, Uehara F, Tazawa H, Toneri M, Hiroshima Y, Yamamoto M, Urata Y, Kagawa S, Bouvet M, Fujiwara T, Hoffman RM. Curative fluorescence-guided cancer surgery of soft-tissue sarcoma in combination with a GFP-labeling oncolytic adeovirus. Oncotarget. 2015;30:13133–13148. doi: 10.18632/oncotarget.3811. - DOI - PMC - PubMed
-
- Yano S, Miwa S, Kishimoto H, Toneri M, Hiroshima Y, Yamamoto M, Bouvet M, Urata Y, Tazawa H, Kagawa S, Fujiwara T, Hoffman RM. Experimental curative fluorescence-guided surgery of highly invasive glioblastoma multiforme selectively labeled with a killer-reporter adenovirus. Mol Ther. 2015;23:1182–1188. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
