

Circulating immune cells in multiple sclerosis
- PMID: 27689339
- PMCID: PMC5217886
- DOI: 10.1111/cei.12878
Circulating immune cells in multiple sclerosis
Abstract
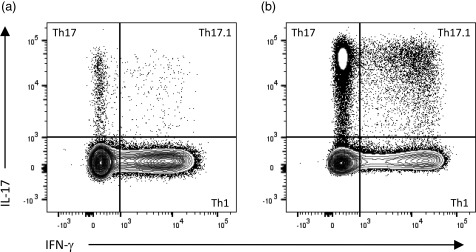
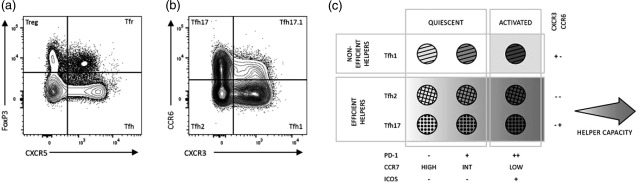
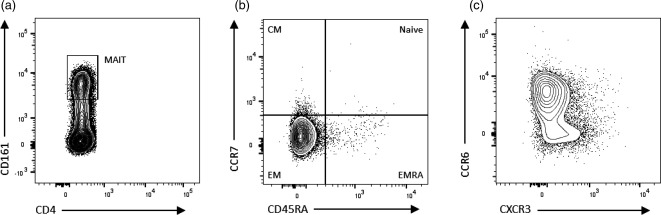
Circulating T and B lymphocytes contribute to the pathogenesis of the neuroinflammatory autoimmune disease, multiple sclerosis (MS). Further progress in the development of MS treatments is dependent upon a greater understanding of the immunological disturbances that underlie the disease. Analyses of circulating immune cells by flow cytometry have revealed MS-associated alterations in the composition and function of T and B cell subsets, including temporal changes associated with disease activity. Disturbances in circulating immune populations reflect those observed in the central nervous system and include skewing towards proinflammatory CD4+ and CD8+ T cells and B cells, greater proportions of follicular T helper cells and functional defects in the corresponding T and B regulatory subsets. Utilizing the analytical power of modern flow cytometers, researchers are now well positioned to monitor immunological changes associated with disease activity or intervention, describe immunological signatures with predictive value and identify targets for therapeutic drug development. This review discusses the contribution of various T and B lymphocyte subsets to MS pathogenesis, provides current and relevant phenotypical descriptions to assist in experimental design and highlights areas of future research.
Keywords: B cells; T cells; flow cytometry; multiple sclerosis.
© 2016 British Society for Immunology.
Figures
References
-
- Koch‐Henriksen N, Sørensen PS. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol 2010; 9:520–32. - PubMed
-
- Salzer J. The only certain measure of the effectiveness of multiple sclerosis therapy is cerebrospinal neurofilament level – YES. Mult Scler 2015; 21:1239–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
