

Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: results from the RA-BUILD study
- PMID: 27689735
- PMCID: PMC5264214
- DOI: 10.1136/annrheumdis-2016-210094
Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: results from the RA-BUILD study
Erratum in
-
Correction: Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: results from the RA-BUILD study.Ann Rheum Dis. 2017 Sep;76(9):1634. doi: 10.1136/annrheumdis-2016-210094corr1. Ann Rheum Dis. 2017. PMID: 28798079 Free PMC article. No abstract available.
Abstract
Background: Baricitinib is an oral, reversible, selective Janus kinase 1 and 2 inhibitor.
Methods: In this phase III, double-blind 24-week study, 684 biologic disease-modifying antirheumatic drug (DMARD)-naïve patients with rheumatoid arthritis and inadequate response or intolerance to ≥1 conventional synthetic DMARDs were randomly assigned 1:1:1 to placebo or baricitinib (2 or 4 mg) once daily, stratified by region and the presence of joint erosions. Endpoint measures included American College of Rheumatology 20% response (ACR20, primary endpoint), Disease Activity Score (DAS28) and Simplified Disease Activity Index (SDAI) score ≤3.3.
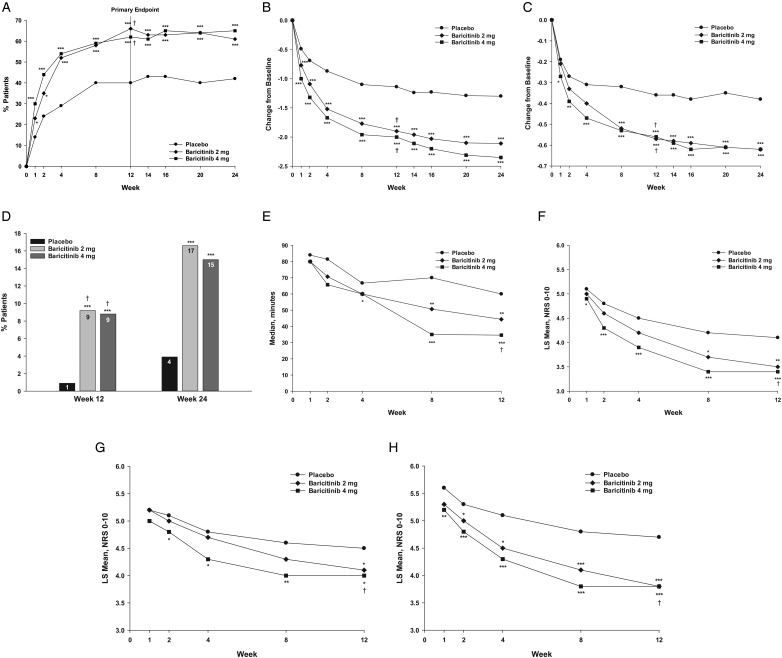
Results: More patients achieved ACR20 response at week 12 with baricitinib 4 mg than with placebo (62% vs 39%, p≤0.001). Compared with placebo, statistically significant improvements in DAS28, SDAI remission, Health Assessment Questionnaire-Disability Index, morning joint stiffness, worst joint pain and worst tiredness were observed. In a supportive analysis, radiographic progression of structural joint damage at week 24 was reduced with baricitinib versus placebo. Rates of adverse events during the treatment period and serious adverse events (SAEs), including serious infections, were similar among groups (SAEs: 5% for baricitinib 4 mg and placebo). One patient had an adverse event of tuberculosis (baricitinib 4 mg); one patient had an adverse event of non-melanoma skin cancer (baricitinib 4 mg). Two deaths and three major adverse cardiovascular events occurred (placebo). Baricitinib was associated with a decrease in neutrophils and increases in low-density and high-density lipoprotein.
Conclusions: In patients with rheumatoid arthritis and an inadequate response or intolerance to conventional synthetic DMARDs, baricitinib was associated with clinical improvement and inhibition of progression of radiographic joint damage.
Trial registration number: NCT01721057; Results.
Keywords: DMARDs (synthetic); Rheumatoid Arthritis; Treatment.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
MD has received grant/research support or consulting support from AbbVie, Bristol Myers Squibb, Eli Lilly and Company, Novartis, Pfizer, Roche, Sanofi and UCB. PE has received grant/research support or consulting support from Abbott, AbbVie, Bristol Myers Squibb, Eli Lilly and Company, MSD, Novartis, Pfizer, Roche, Samsung, Takeda and UCB. DvdH has received grant/research support and/or consulting fees from AbbVie, Amgen, AstraZeneca, Augurex, Bristol Myers Squibb, Boehringer Ingelheim, Celgene, Centocor, Chugai, Covagen, Daiichi, Eli Lilly and Company, Galapagos, Glaxo-Smith Kline, Janssen Biologics, Merck, Novartis, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi, UCB and Vertex and is director of Imaging Rheumatology bv. Y-CC has received speakers bureau fees and/or grant research support from AbbVie, Bristol Myers Squibb, Eli Lilly and Company and Pfizer. MG received research support from Eli Lilly and Company. JL, SB, SW, IdlT, CG, TR, DS and SdB are employees of Eli Lilly and Company and may own stock or stock options in Eli Lilly and Company.
Figures


References
-
- Tanaka Y, Emoto K, Tsujimoto M, et al. 12-week results of a phase 2b dose-ranging study of baricitinib, an oral JAK1/JAK2 inhibitor in Japanese patients with rheumatoid arthritis on background methotrexate therapy. Arthritis Rheum 2013;65:S765.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
