

Pediatric Idiopathic Intracranial Hypertension: Age, Gender, and Anthropometric Features at Diagnosis in a Large, Retrospective, Multisite Cohort
- PMID: 27692528
- PMCID: PMC5257253
- DOI: 10.1016/j.ophtha.2016.08.004
Pediatric Idiopathic Intracranial Hypertension: Age, Gender, and Anthropometric Features at Diagnosis in a Large, Retrospective, Multisite Cohort
Abstract
Purpose: To examine anthropometric and maturational characteristics at diagnosis in pediatric idiopathic intracranial hypertension (IIH).
Design: Retrospective, international, multisite study.
Participants: Pediatric patients (2-18 years of age at diagnosis) with IIH.
Main outcome measures: Body mass index (BMI), height, and weight Z-scores; sexual maturation.
Methods: Cases of IIH were identified retrospectively based on diagnostic code, pediatric neuro-ophthalmologist databases, or both and updated diagnostic criteria (2013) were applied to confirm definite IIH. Anthropometric measurements were converted into age- and gender-specific height, weight, and BMI Z-scores CDC 2000 growth charts. When available, sexual maturation was noted.
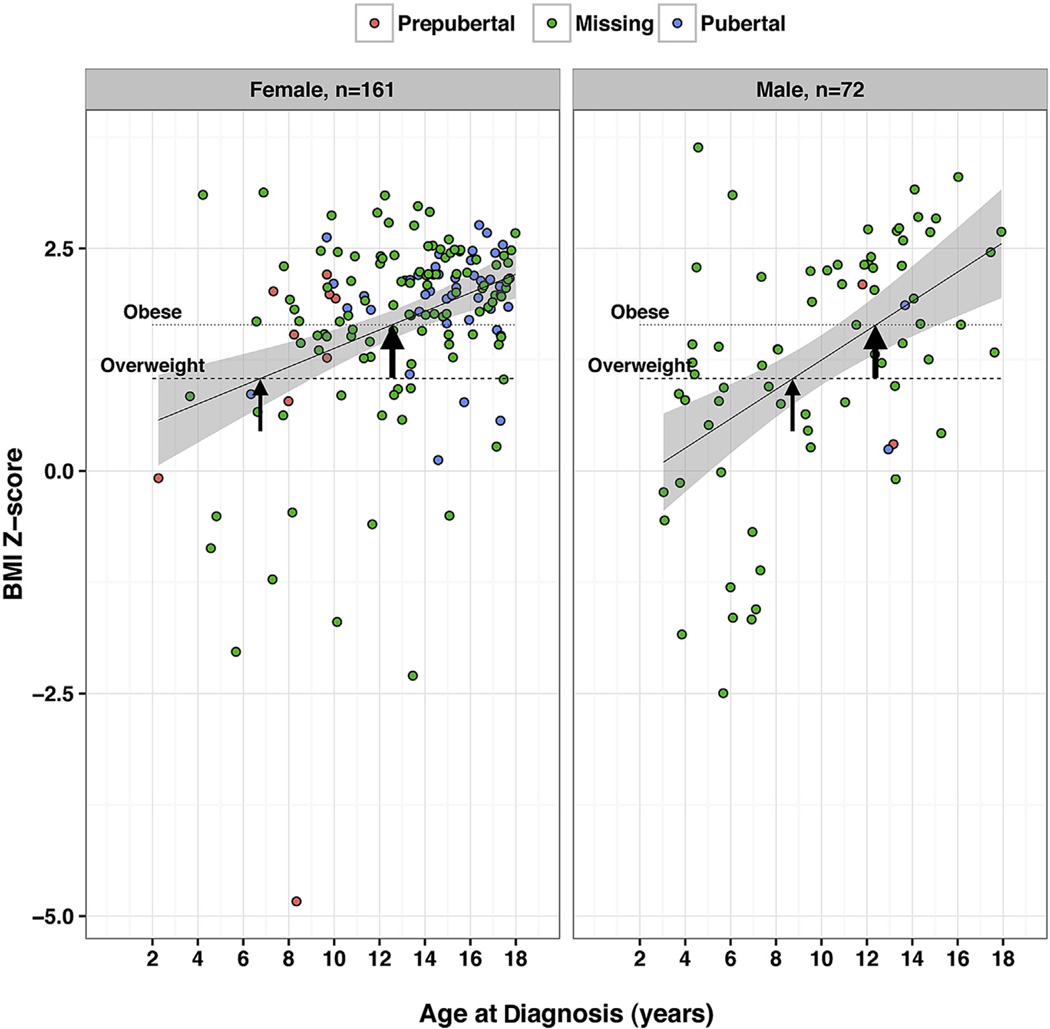
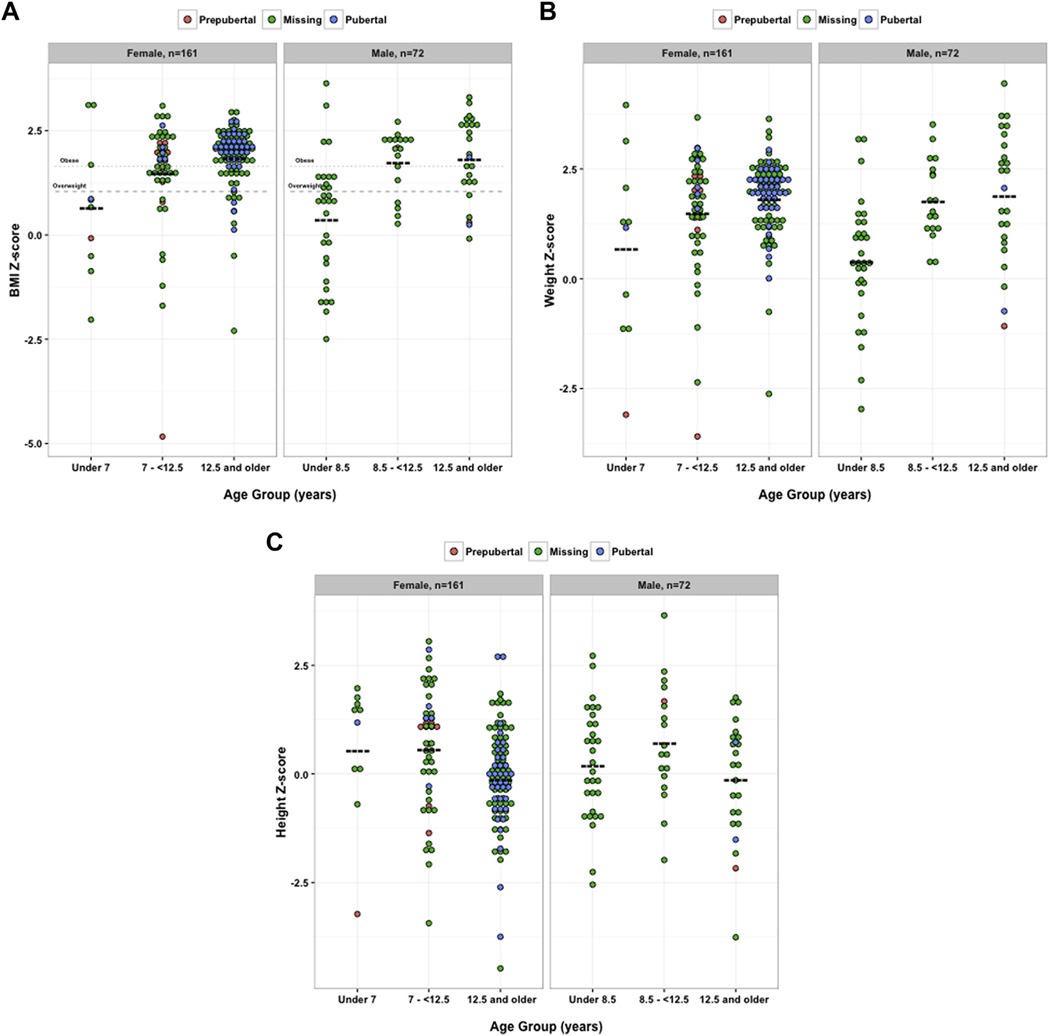
Results: Two hundred thirty-three cases of definite IIH were identified across 8 sites. In boys, a moderate association between age and BMI Z-scores was noted (Pearson's correlation coefficient, 0.50; 95% confidence interval [CI], 0.30-0.66; P < 0.001; n = 72), and in girls, a weak association was noted (Pearson's correlation coefficient, 0.34; 95% CI, 0.20-0.47; P < 0.001; n = 161). The average patient was more likely to be overweight at diagnosis at age 6.7 years in girls and 8.7 years in boys, and obese at diagnosis at age 12.5 years in girls and 12.4 years in boys. Compared with age- and gender-matched reference values, early adolescent patients were taller for age (P = 0.002 in girls and P = 0.02 in boys). Data on Tanner staging, menarchal status, or both were available in 25% of cases (n = 57/233). Prepubertal participants (n = 12) had lower average BMI Z-scores (0.95±1.98) compared with pubertal participants (n = 45; 1.92±0.60), but this result did not reach statistical significance (P = 0.09).
Conclusions: With updated diagnostic criteria and pediatric-specific assessments, the present study identifies 3 subgroups of pediatric IIH: a young group that is not overweight, an early adolescent group that is either overweight or obese, and a late adolescent group that is mostly obese. Data also suggest that the early adolescent group with IIH may be taller than age- and gender-matched reference values. Understanding these features of pediatric IIH may help to illuminate the complex pathogenesis of this condition.
Copyright © 2016 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013;81:1–7. - PubMed
-
- Balcer LJ, Liu GT, Forman S, et al. Idiopathic intracranial hypertension: relation of age and obesity in children. Neurology. 1999;52(4):870–872. - PubMed
-
- Ko MW, Liu GT. Pediatric idiopathic intracranial hypertension (pseudotumor cerebri) Horm Res Paediatr. 2010;74(6):381–389. - PubMed
-
- Rangwala LM, Liu GT. Pediatric idiopathic intracranial hypertension. Surv Ophthalmol. 2007;52(6):597–617. - PubMed
-
- Cinciripini GS, Donahue S, Borchert MS. Idiopathic intracranial hypertension in prepubertal pediatric patients: characteristics, treatment, and outcome. Am J Ophthalmol. 1999;127(2):178–182. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
