

The Effect of Combined Out-of-Hospital Hypotension and Hypoxia on Mortality in Major Traumatic Brain Injury
- PMID: 27692683
- PMCID: PMC5173421
- DOI: 10.1016/j.annemergmed.2016.08.007
The Effect of Combined Out-of-Hospital Hypotension and Hypoxia on Mortality in Major Traumatic Brain Injury
Abstract
Study objective: Survival is significantly reduced by either hypotension or hypoxia during the out-of-hospital management of major traumatic brain injury. However, only a handful of small studies have investigated the influence of the combination of both hypotension and hypoxia occurring together. In patients with major traumatic brain injury, we evaluate the associations between mortality and out-of-hospital hypotension and hypoxia separately and in combination.
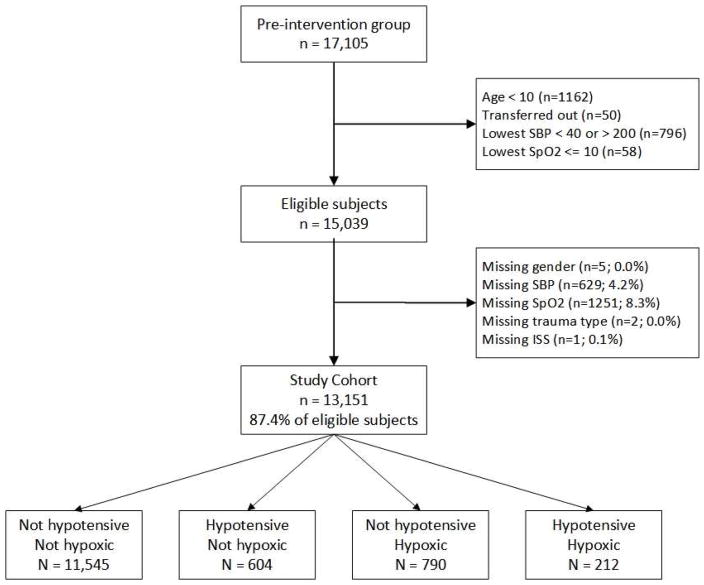
Methods: All moderate or severe traumatic brain injury cases in the preimplementation cohort of the Excellence in Prehospital Injury Care study (a statewide, before/after, controlled study of the effect of implementing the out-of-hospital traumatic brain injury treatment guidelines) from January 1, 2007, to March 31, 2014, were evaluated (exclusions: <10 years, out-of-hospital oxygen saturation ≤10%, and out-of-hospital systolic blood pressure <40 or >200 mm Hg). The relationship between mortality and hypotension (systolic blood pressure <90 mm Hg) or hypoxia (saturation <90%) was assessed with multivariable logistic regression, controlling for Injury Severity Score, head region severity, injury type (blunt versus penetrating), age, sex, race, ethnicity, payer, interhospital transfer, and trauma center.
Results: Among the 13,151 patients who met inclusion criteria (median age 45 years; 68.6% men), 11,545 (87.8%) had neither hypotension nor hypoxia, 604 (4.6%) had hypotension only, 790 (6.0%) had hypoxia only, and 212 (1.6%) had both hypotension and hypoxia. Mortality for the 4 study cohorts was 5.6%, 20.7%, 28.1%, and 43.9%, respectively. The crude and adjusted odds ratios for death within the cohorts, using the patients with neither hypotension nor hypoxia as the reference, were 4.4 and 2.5, 6.6 and 3.0, and 13.2 and 6.1, respectively. Evaluation for an interaction between hypotension and hypoxia revealed that the effects were additive on the log odds of death.
Conclusion: In this statewide analysis of major traumatic brain injury, combined out-of-hospital hypotension and hypoxia were associated with significantly increased mortality. This effect on survival persisted even after controlling for multiple potential confounders. In fact, the adjusted odds of death for patients with both hypotension and hypoxia were more than 2 times greater than for those with either hypotension or hypoxia alone. These findings seem supportive of the emphasis on aggressive prevention and treatment of hypotension and hypoxia reflected in the current emergency medical services traumatic brain injury treatment guidelines but clearly reveal the need for further study to determine their influence on outcome.
Trial registration: ClinicalTrials.gov NCT01339702.
Copyright © 2016 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Words Matter: Researchers Should Avoid Implying Causation in Studies of Association.Ann Emerg Med. 2017 Aug;70(2):262-263. doi: 10.1016/j.annemergmed.2017.03.016. Ann Emerg Med. 2017. PMID: 28734472 No abstract available.
-
In reply.Ann Emerg Med. 2017 Aug;70(2):263-264. doi: 10.1016/j.annemergmed.2017.03.015. Ann Emerg Med. 2017. PMID: 28734473 No abstract available.
References
-
- Finkelstein E, Corso PS, Miller TR. The incidence and economic burden of injuries in the United States. Oxford ; New York: Oxford University Press; 2006.
-
- Bell JMBM, Jenkins EL, Haarbauer-Krupa J. Traumatic Brain Injury In the United States: Epidemiology and Rehabilitation. National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention, Centers for Disease Control; ; 2014.
-
- Thurman DJ, Alverson C, Dunn KA, Guerrero J, Sniezek JE. Traumatic brain injury in the United States: A public health perspective. J Head Trauma Rehabil. 1999;14(6):602–615. - PubMed
-
- Davis DP, Fakhry SM, Wang HE, et al. Paramedic rapid sequence intubation for severe traumatic brain injury: perspectives from an expert panel. Prehosp Emerg Care. 2007;11(1):1–8. - PubMed
-
- Davis DP, Idris AH, Sise MJ, et al. Early ventilation and outcome in patients with moderate to severe traumatic brain injury. Crit Care Med. 2006;34(4):1202–1208. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
