

Trends in Receipt of Intensive Procedures at the End of Life Among Patients Treated With Maintenance Dialysis
- PMID: 27693262
- PMCID: PMC5182121
- DOI: 10.1053/j.ajkd.2016.07.028
Trends in Receipt of Intensive Procedures at the End of Life Among Patients Treated With Maintenance Dialysis
Abstract
Background: Many dialysis patients receive intensive procedures intended to prolong life at the very end of life. However, little is known about trends over time in the use of these procedures. We describe temporal trends in receipt of inpatient intensive procedures during the last 6 months of life among patients treated with maintenance dialysis.
Study design: Mortality follow-back study.
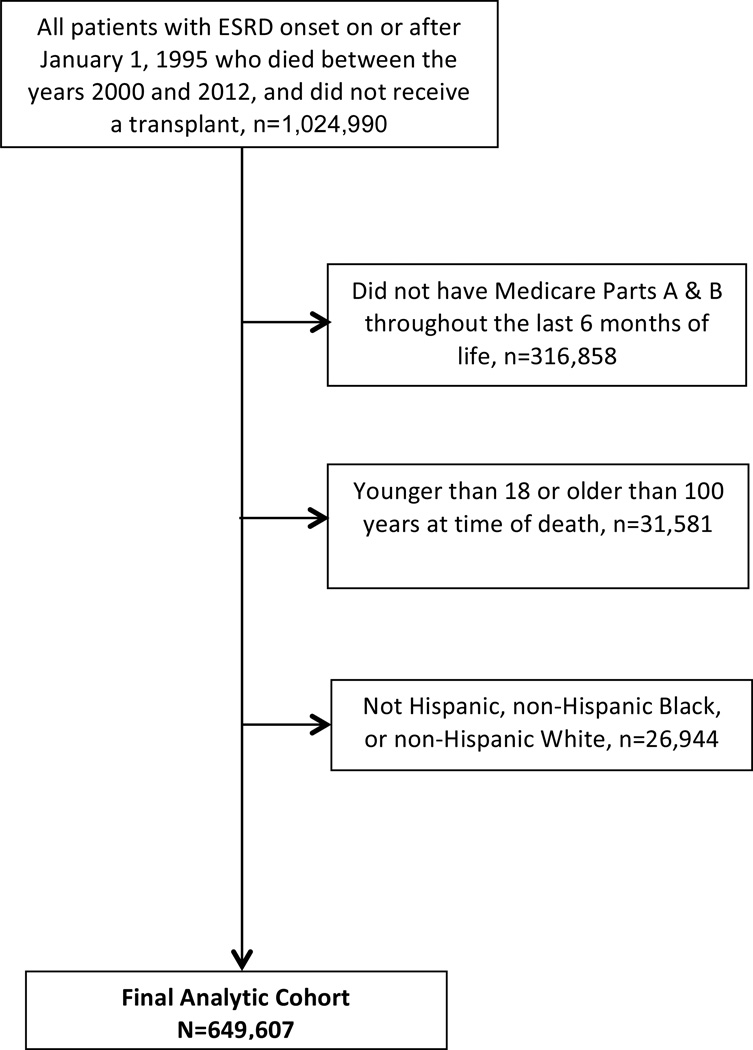
Setting & participants: 649,607 adult Medicare beneficiaries on maintenance dialysis therapy who died in 2000 to 2012.
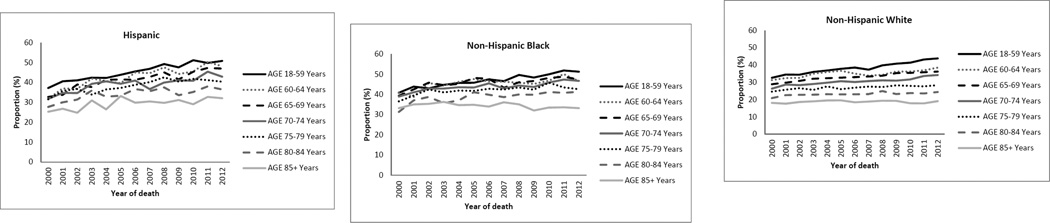
Predictors: Period of death (2000-2003, 2004-2008, or 2009-2012), age at time of death (18-59, 60-64, 65-69, 70-74, 75-79, 80-84, and ≥85 years), and race/ethnicity (Hispanic, non-Hispanic black, or non-Hispanic white).
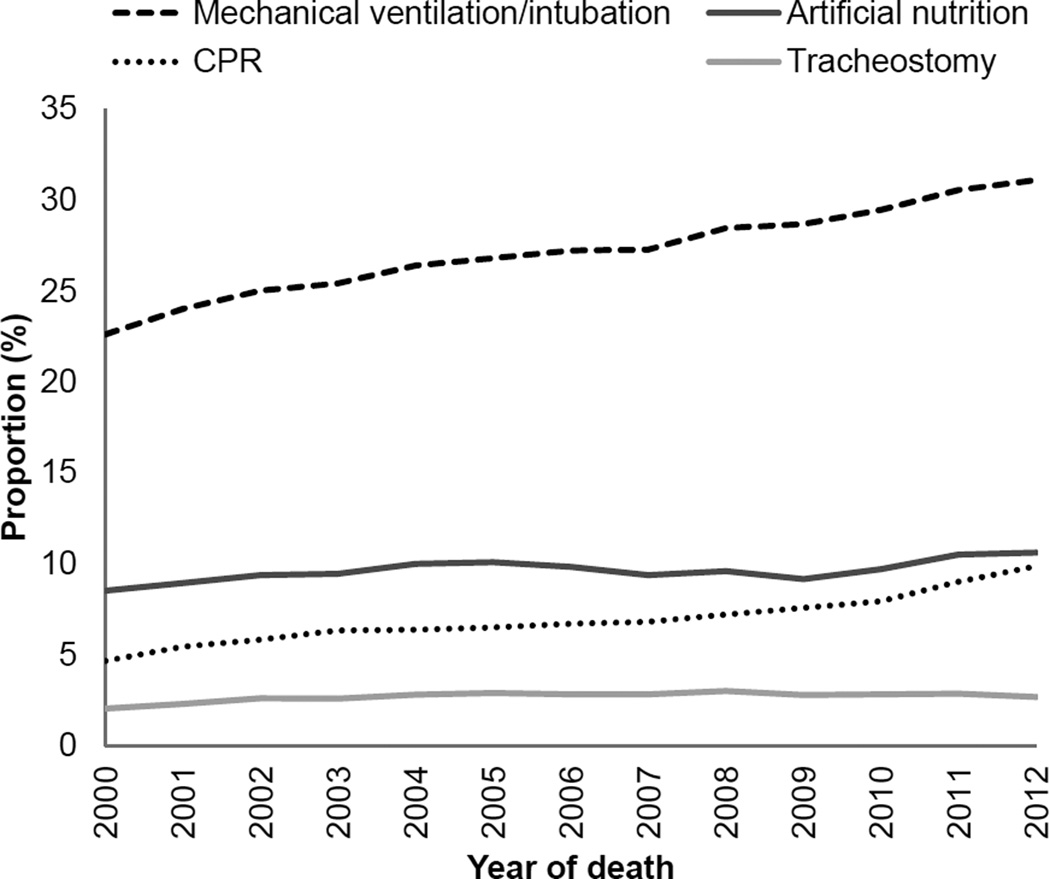
Outcome: Receipt of an inpatient intensive procedure (defined as invasive mechanical ventilation/intubation, tracheostomy, gastrostomy/jejunostomy tube insertion, enteral or parenteral nutrition, or cardiopulmonary resuscitation) during the last 6 months of life.
Results: Overall, 34% of cohort patients received an intensive procedure in the last 6 months of life, increasing from 29% in 2000 to 36% in 2012 (with 2000-2003 as the referent category; adjusted risk ratios [RRs] were 1.06 [95% CI, 1.05-1.07] and 1.10 [95% CI, 1.09-1.12] for 2004-2008 and 2009-2012, respectively). Use of intensive procedures increased more markedly over time in younger versus older patients (comparing 2009-2012 to 2000-2003, adjusted RR was 1.18 [95% CI, 1.15-1.20] for the youngest age group as opposed to 1.00 [95% CI, 0.96-1.04] for the oldest group). Comparing 2009 to 2012 to 2000 to 2003, the use of intensive procedures increased more dramatically for Hispanic patients than for non-Hispanic black or non-Hispanic white patients (adjusted RRs of 1.18 [95% CI, 1.14-1.22], 1.09 [95% CI, 1.07-1.11], and 1.10 [95% CI, 1.08-1.12], respectively).
Limitations: Data sources do not provide insight into reasons for observed trends in the use of intensive procedures.
Conclusions: Among patients treated with maintenance dialysis, there is a trend toward more frequent use of intensive procedures at the end of life, especially in younger patients and those of Hispanic ethnicity.
Keywords: End-of-life; Hispanic; Medicare spending; age differences; dialysis; elderly; end-stage renal disease (ESRD); ethnic disparities; health care costs; hospitalization; intensive procedures; mortality follow-back.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Pasternak S. End-of-Life Care Constitutes Third Rail of U.S. Health Care Policy Debate. 2013
-
- Fisher ES, Wennberg DE, Stukel TA, Gottlieb DJ, Lucas FL, Pinder EL. The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Annals of internal medicine. 2003;138:288–298. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
