

Prediction of Sepsis in the Intensive Care Unit With Minimal Electronic Health Record Data: A Machine Learning Approach
- PMID: 27694098
- PMCID: PMC5065680
- DOI: 10.2196/medinform.5909
Prediction of Sepsis in the Intensive Care Unit With Minimal Electronic Health Record Data: A Machine Learning Approach
Abstract
Background: Sepsis is one of the leading causes of mortality in hospitalized patients. Despite this fact, a reliable means of predicting sepsis onset remains elusive. Early and accurate sepsis onset predictions could allow more aggressive and targeted therapy while maintaining antimicrobial stewardship. Existing detection methods suffer from low performance and often require time-consuming laboratory test results.
Objective: To study and validate a sepsis prediction method, InSight, for the new Sepsis-3 definitions in retrospective data, make predictions using a minimal set of variables from within the electronic health record data, compare the performance of this approach with existing scoring systems, and investigate the effects of data sparsity on InSight performance.
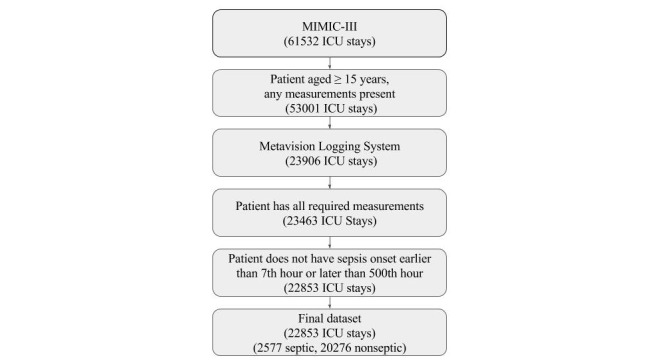
Methods: We apply InSight, a machine learning classification system that uses multivariable combinations of easily obtained patient data (vitals, peripheral capillary oxygen saturation, Glasgow Coma Score, and age), to predict sepsis using the retrospective Multiparameter Intelligent Monitoring in Intensive Care (MIMIC)-III dataset, restricted to intensive care unit (ICU) patients aged 15 years or more. Following the Sepsis-3 definitions of the sepsis syndrome, we compare the classification performance of InSight versus quick sequential organ failure assessment (qSOFA), modified early warning score (MEWS), systemic inflammatory response syndrome (SIRS), simplified acute physiology score (SAPS) II, and sequential organ failure assessment (SOFA) to determine whether or not patients will become septic at a fixed period of time before onset. We also test the robustness of the InSight system to random deletion of individual input observations.
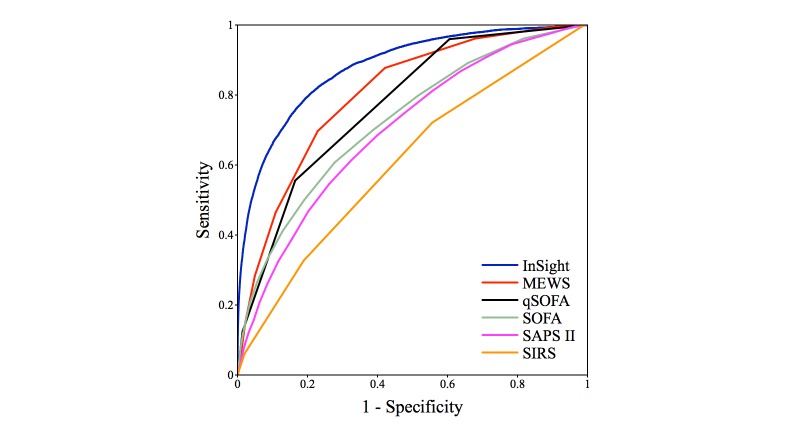
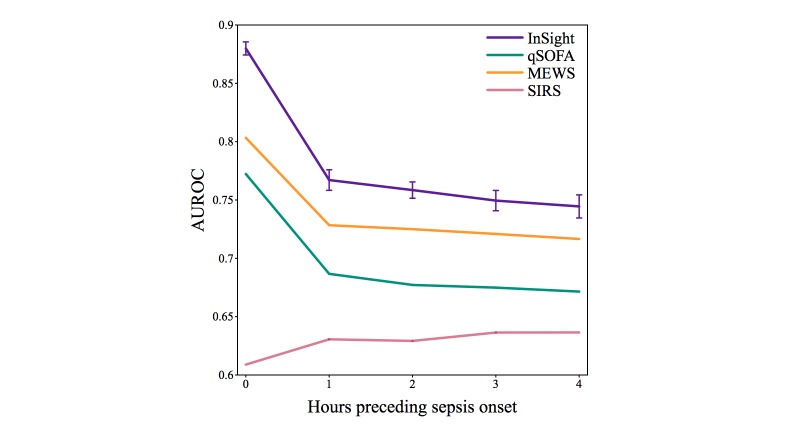
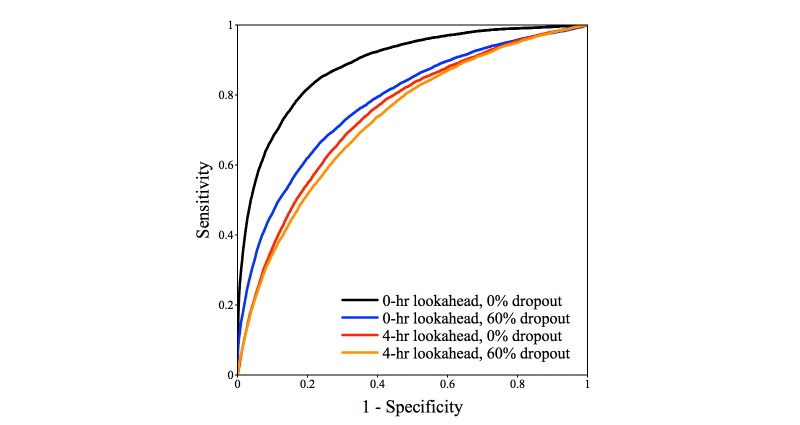
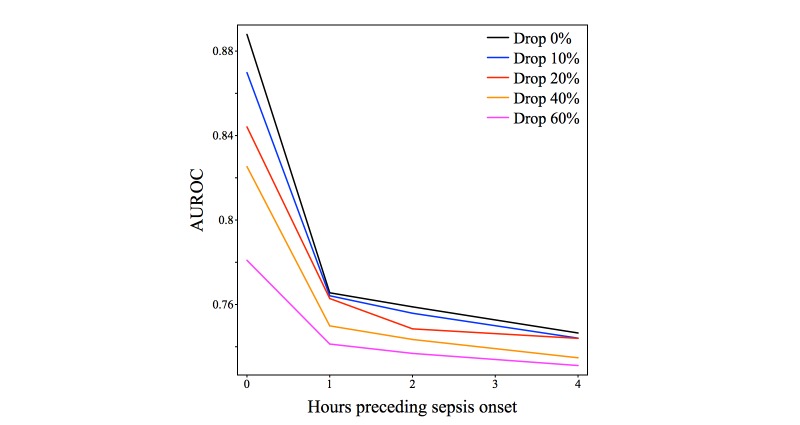
Results: In a test dataset with 11.3% sepsis prevalence, InSight produced superior classification performance compared with the alternative scores as measured by area under the receiver operating characteristic curves (AUROC) and area under precision-recall curves (APR). In detection of sepsis onset, InSight attains AUROC = 0.880 (SD 0.006) at onset time and APR = 0.595 (SD 0.016), both of which are superior to the performance attained by SIRS (AUROC: 0.609; APR: 0.160), qSOFA (AUROC: 0.772; APR: 0.277), and MEWS (AUROC: 0.803; APR: 0.327) computed concurrently, as well as SAPS II (AUROC: 0.700; APR: 0.225) and SOFA (AUROC: 0.725; APR: 0.284) computed at admission (P<.001 for all comparisons). Similar results are observed for 1-4 hours preceding sepsis onset. In experiments where approximately 60% of input data are deleted at random, InSight attains an AUROC of 0.781 (SD 0.013) and APR of 0.401 (SD 0.015) at sepsis onset time. Even with 60% of data missing, InSight remains superior to the corresponding SIRS scores (AUROC and APR, P<.001), qSOFA scores (P=.0095; P<.001) and superior to SOFA and SAPS II computed at admission (AUROC and APR, P<.001), where all of these comparison scores (except InSight) are computed without data deletion.
Conclusions: Despite using little more than vitals, InSight is an effective tool for predicting sepsis onset and performs well even with randomly missing data.
Keywords: clinical decision support systems; electronic health records; machine learning; medical informatics; sepsis.
Conflict of interest statement
All authors who have affiliations listed with Dascena (Hayward, CA, USA) are employees of Dascena.
Figures



References
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, Angus DC, Reinhart K, International Forum of Acute Care Trialists Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am J Respir Crit Care Med. 2016 Feb 1;193(3):259–72. doi: 10.1164/rccm.201504-0781OC. - DOI - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001 Jul;29(7):1303–10. - PubMed
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche J, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent J, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016 Feb 23;315(8):801–10. doi: 10.1001/jama.2016.0287.2492881 - DOI - PMC - PubMed
-
- Vincent JL, Moreno R, Takala J, Willatts S, De MA, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996 Jul;22(7):707–10. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
