

Anterior Shoulder Instability in the Military Athlete
- PMID: 27694151
- PMCID: PMC5089361
- DOI: 10.1177/1941738116672161
Anterior Shoulder Instability in the Military Athlete
Abstract
Context: Given its young, predominately male demographics and intense physical demands, the US military remains an ideal cohort for the study of anterior shoulder instability.
Evidence acquisition: A literature search of PubMed, MEDLINE, and the Cochrane Database was performed to identify all peer-reviewed publications from 1950 to 2016 from US military orthopaedic surgeons focusing on the management of anterior shoulder instability.
Study design: Clinical review.
Level of evidence: Level 4.
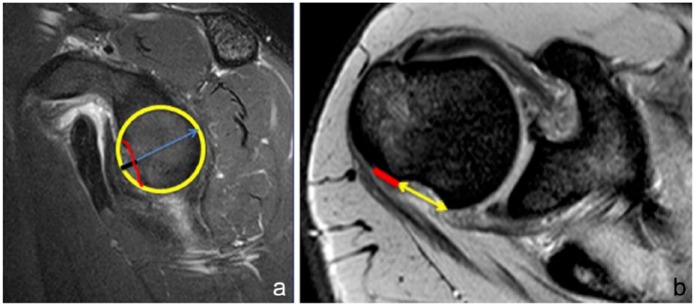
Results: The incidence of anterior shoulder instability events in the military occurs at an order of magnitude greater than in civilian populations, with rates as high as 3% per year among high-risk groups. With more than 90% risk of a Bankart lesion and high risk for instability recurrence, the military has advocated for early intervention of first-time shoulder instability while documenting up to 76% relative risk reduction versus nonoperative treatment. Preoperative evaluation with advanced radiographic imaging should be used to evaluate for attritional bone loss or "off-track" engaging defects to guide comprehensive surgical management. With complex recurrent shoulder instability and/or cases of clinically significant osseous lesions, potential options such as remplissage, anterior open capsular procedures, or bone augmentation procedures may be preferentially considered.
Conclusion: Careful risk stratification, clinical evaluation, and selective surgical management for at-risk military patients with anterior shoulder instability can optimize the recurrence risk and functional outcome in this population.
Keywords: anterior; dislocation; military; shoulder instability; subluxation.
Conflict of interest statement
The following authors declared potential conflicts of interest: Brett D. Owens, MD, is a paid consultant for MTF/Conmed and Mitek and receives royalties from Springer, Elsevier, and Slack. John M. Tokish, MD, is a paid consultant for Arthrex and Dupey-Mitek.
Figures

References
-
- Arciero RA, Parrino A, Bernhardson AS, et al. The effect of a combined glenoid and Hill-Sachs defect on glenohumeral stability: a biomechanical cadaveric study using 3-dimensional modeling of 142 patients. Am J Sports Med. 2015;43:1422-1429. - PubMed
-
- Arciero RA, Wheeler JH, Ryan JB, McBride JT. Arthroscopic Bankart repair versus nonoperative treatment for acute, initial anterior shoulder dislocations. Am J Sports Med. 1994;22:589-594. - PubMed
-
- Balg F, Boileau P. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br. 2007;89:1470-1477. - PubMed
-
- Belmont PJ Jr, Goodman GP, Waterman B, DeZee K, Burks R, Owens BD. Disease and nonbattle injuries sustained by a U.S. Army Brigade Combat Team during Operation Iraqi Freedom. Mil Med. 2010;175:469-476. - PubMed
-
- Bernhardson AS, Bailey JR, Solomon DJ, Stanley M, Provencher MT. Glenoid bone loss in the setting of an anterior labroligamentous periosteal sleeve avulsion tear. Am J Sports Med. 2014;42:2136-2140. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
