

Peripheral blood mononuclear cell secretome for tissue repair
- PMID: 27696124
- PMCID: PMC5082595
- DOI: 10.1007/s10495-016-1292-8
Peripheral blood mononuclear cell secretome for tissue repair
Abstract
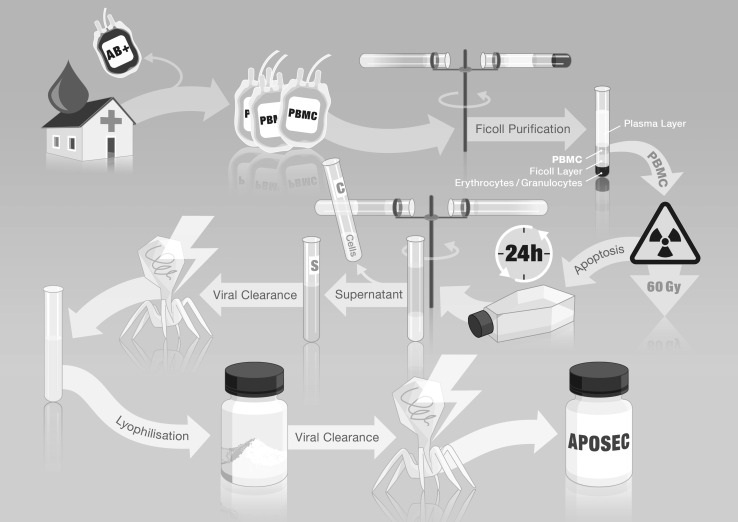
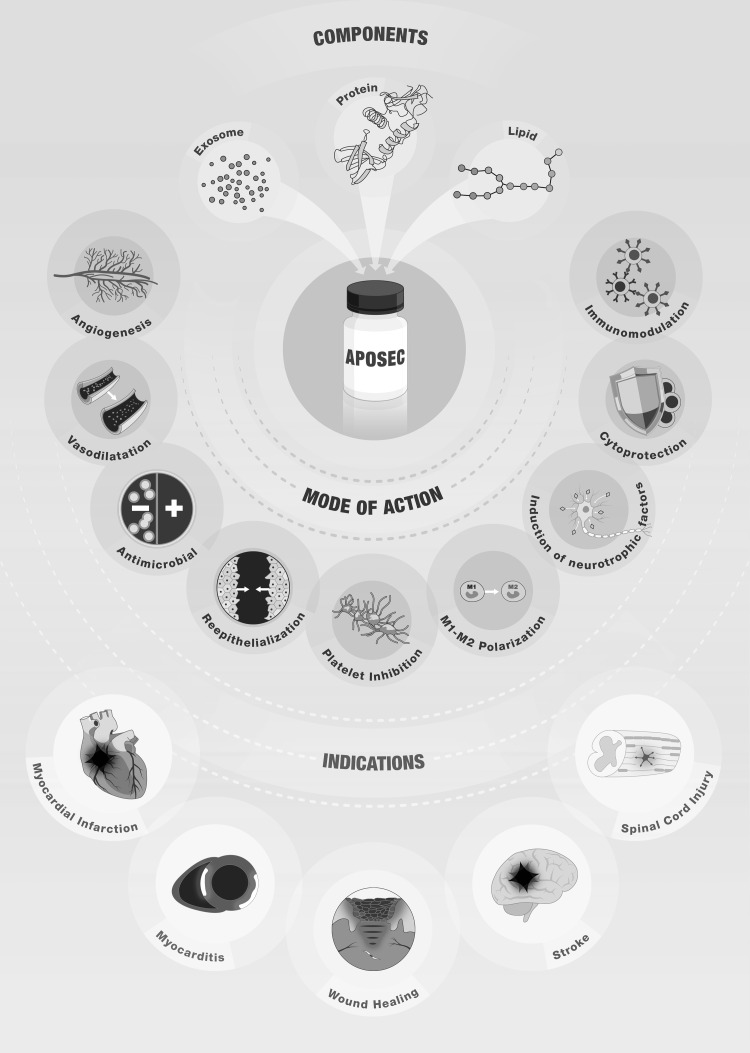
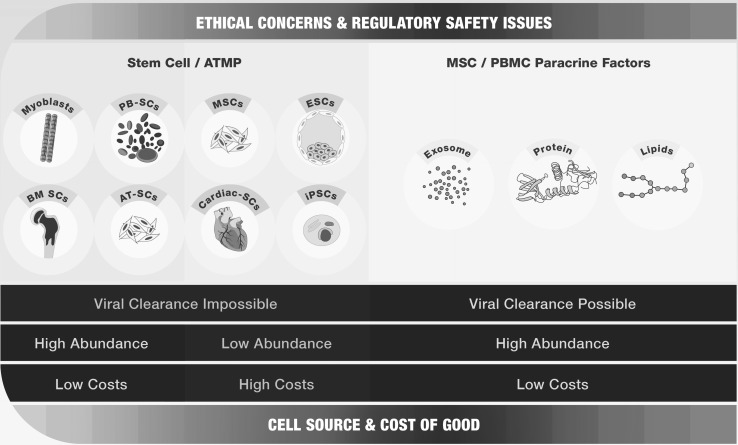
For almost two decades, cell-based therapies have been tested in modern regenerative medicine to either replace or regenerate human cells, tissues, or organs and restore normal function. Secreted paracrine factors are increasingly accepted to exert beneficial biological effects that promote tissue regeneration. These factors are called the cell secretome and include a variety of proteins, lipids, microRNAs, and extracellular vesicles, such as exosomes and microparticles. The stem cell secretome has most commonly been investigated in pre-clinical settings. However, a growing body of evidence indicates that other cell types, such as peripheral blood mononuclear cells (PBMCs), are capable of releasing significant amounts of biologically active paracrine factors that exert beneficial regenerative effects. The apoptotic PBMC secretome has been successfully used pre-clinically for the treatment of acute myocardial infarction, chronic heart failure, spinal cord injury, stroke, and wound healing. In this review we describe the benefits of choosing PBMCs instead of stem cells in regenerative medicine and characterize the factors released from apoptotic PBMCs. We also discuss pre-clinical studies with apoptotic cell-based therapies and regulatory issues that have to be considered when conducting clinical trials using cell secretome-based products. This should allow the reader to envision PBMC secretome-based therapies as alternatives to all other forms of cell-based therapies.
Keywords: PBMC; Paracrine; Regenerative medicine; Secretome; Tissue regeneration.
Conflict of interest statement
The Medical University of Vienna has claimed financial interest. Aposcience AG holds patents related to this work (EP20080450198 and EP20080450199). HJA is a shareholder of Aposcience AG. All other authors declare no potential conflicts of interest.
Figures

References
-
- Niehans P. 20 Jahre Zellular-Therapie. Berlin: Urban & Schwarzenberg; 1952. - PubMed
-
- Rietschel H. Frischzellentherapie und ihre Gefharen. Wiener Med Wochenschr. 1955;46:949–957. - PubMed
-
- Maximow AA (1909) Der lymphozyt als gemeinsame stammzelle der verschiedenen blutelement in der embryonalen entwicklung und im postfetalen leben der säugetiere. Folia Haematologica 8
-
- Metchnikoff II. The prolongation of life: optimistic studies. New York: Springer; 2004.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
