

Deciphering KRAS and NRAS mutated clone dynamics in MLL-AF4 paediatric leukaemia by ultra deep sequencing analysis
- PMID: 27698462
- PMCID: PMC5048141
- DOI: 10.1038/srep34449
Deciphering KRAS and NRAS mutated clone dynamics in MLL-AF4 paediatric leukaemia by ultra deep sequencing analysis
Abstract
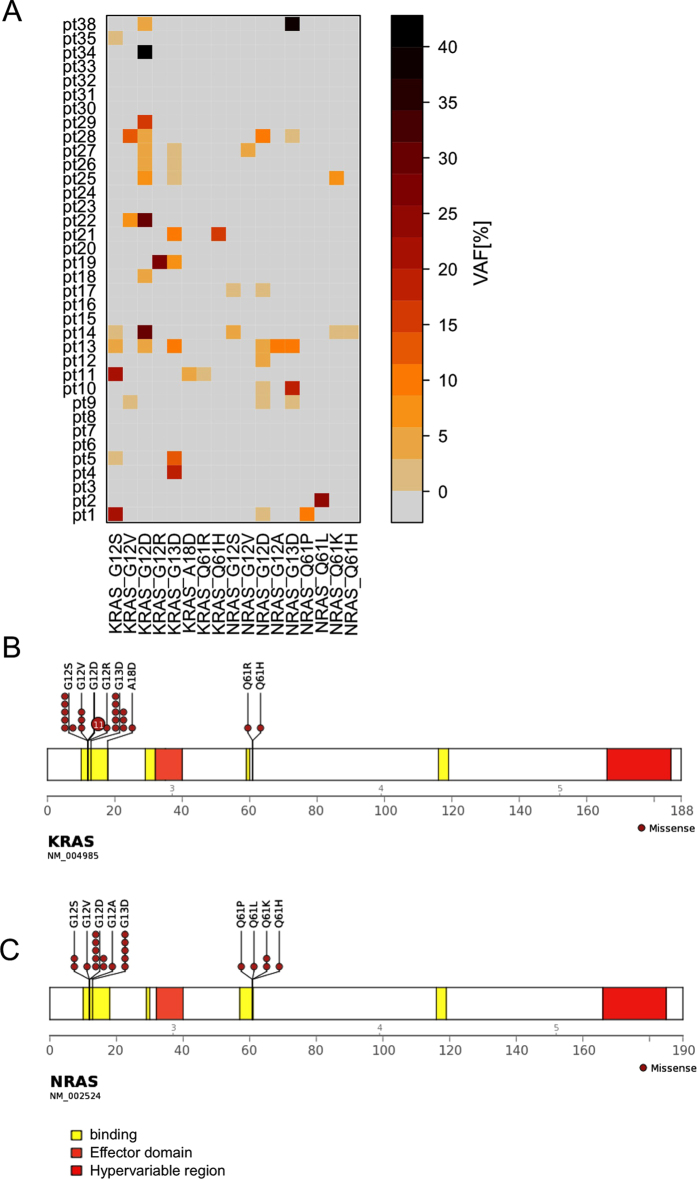
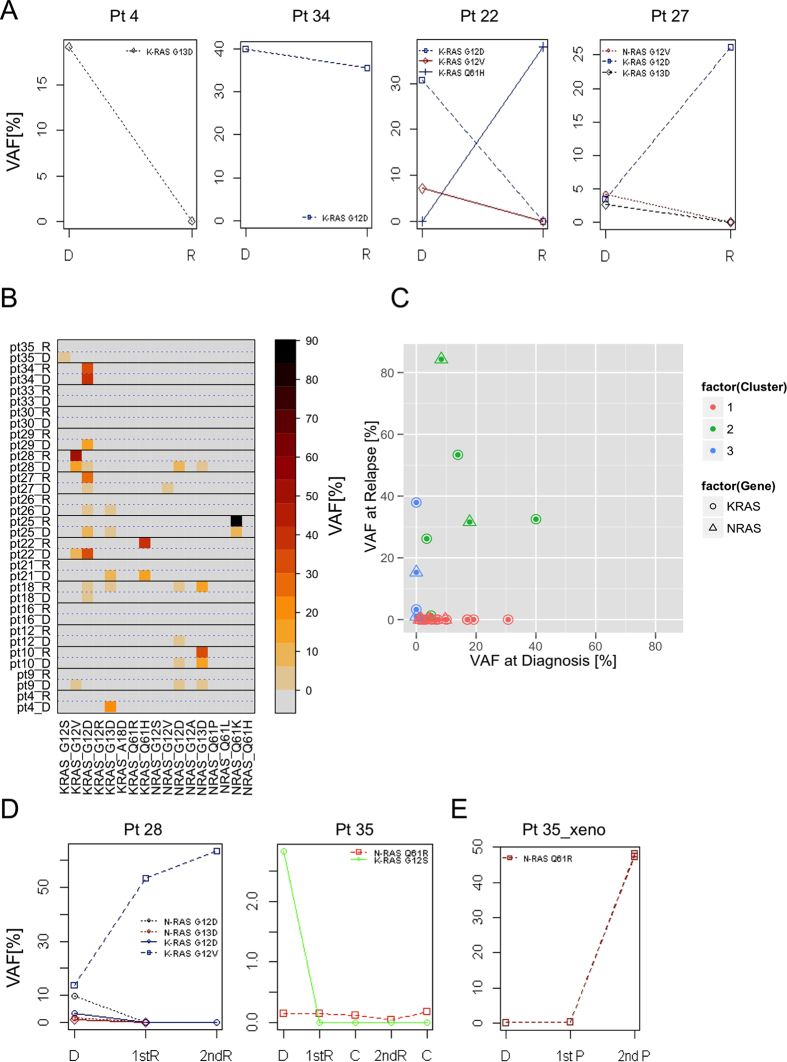
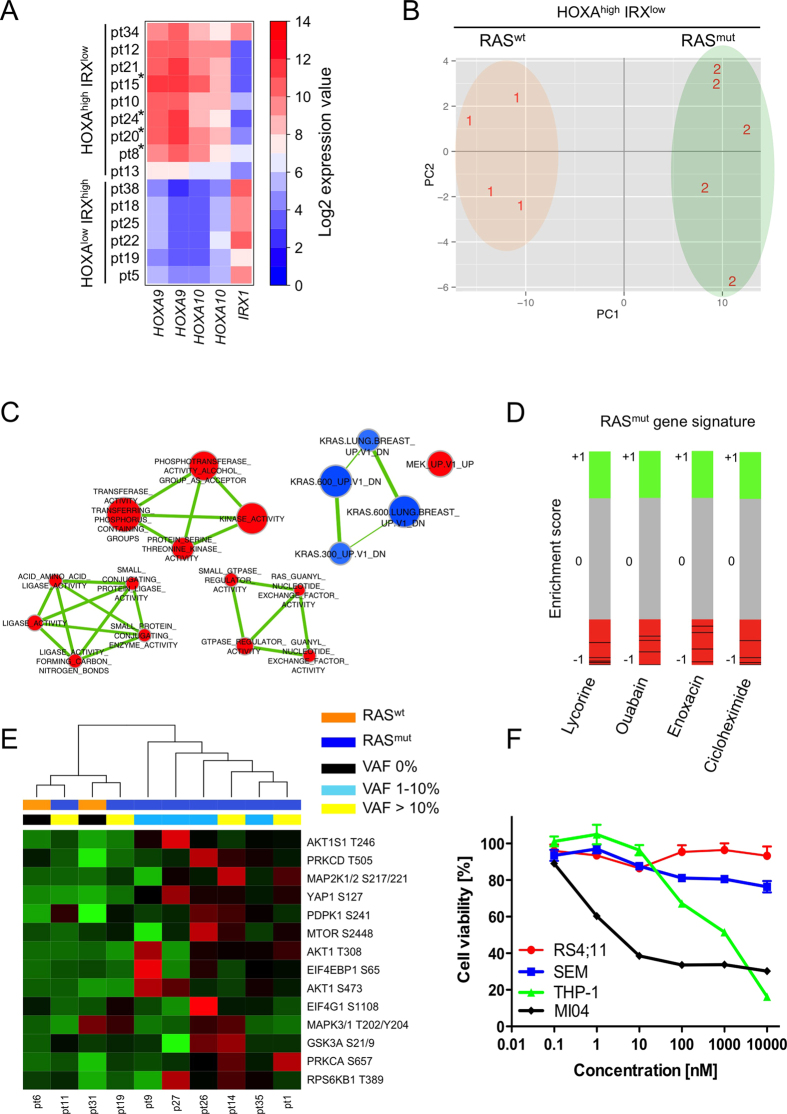
To induce and sustain the leukaemogenic process, MLL-AF4+ leukaemia seems to require very few genetic alterations in addition to the fusion gene itself. Studies of infant and paediatric patients with MLL-AF4+ B cell precursor acute lymphoblastic leukaemia (BCP-ALL) have reported mutations in KRAS and NRAS with incidences ranging from 25 to 50%. Whereas previous studies employed Sanger sequencing, here we used next generation amplicon deep sequencing for in depth evaluation of RAS mutations in 36 paediatric patients at diagnosis of MLL-AF4+ leukaemia. RAS mutations including those in small sub-clones were detected in 63.9% of patients. Furthermore, the mutational analysis of 17 paired samples at diagnosis and relapse revealed complex RAS clone dynamics and showed that the mutated clones present at relapse were almost all originated from clones that were already detectable at diagnosis and survived to the initial therapy. Finally, we showed that mutated patients were indeed characterized by a RAS related signature at both transcriptional and protein levels and that the targeting of the RAS pathway could be of beneficial for treatment of MLL-AF4+ BCP-ALL clones carrying somatic RAS mutations.
Figures
References
-
- Pui C. H. et al. Clinical heterogeneity in childhood acute lymphoblastic leukemia with 11q23 rearrangements. Leukemia 17, 700–706 (2003). - PubMed
-
- Mann G. et al. Improved outcome with hematopoietic stem cell transplantation in a poor prognostic subgroup of infants with mixed-lineage-leukemia (MLL)-rearranged acute lymphoblastic leukemia: results from the Interfant-99 Study. Blood 116, 2644–2650 (2010). - PubMed
-
- Ayton P. M. & Cleary M. L. Molecular mechanisms of leukemogenesis mediated by MLL fusion proteins. Oncogene 20, 5695–5707 (2001). - PubMed
-
- Krivtsov A. V. & Armstrong S. A. MLL translocations, histone modifications and leukaemia stem-cell development. Nat. Rev. Cancer. 7, 823–833 (2007). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
