

Anti-tubulin drugs conjugated to anti-ErbB antibodies selectively radiosensitize
- PMID: 27698471
- PMCID: PMC5059467
- DOI: 10.1038/ncomms13019
Anti-tubulin drugs conjugated to anti-ErbB antibodies selectively radiosensitize
Abstract
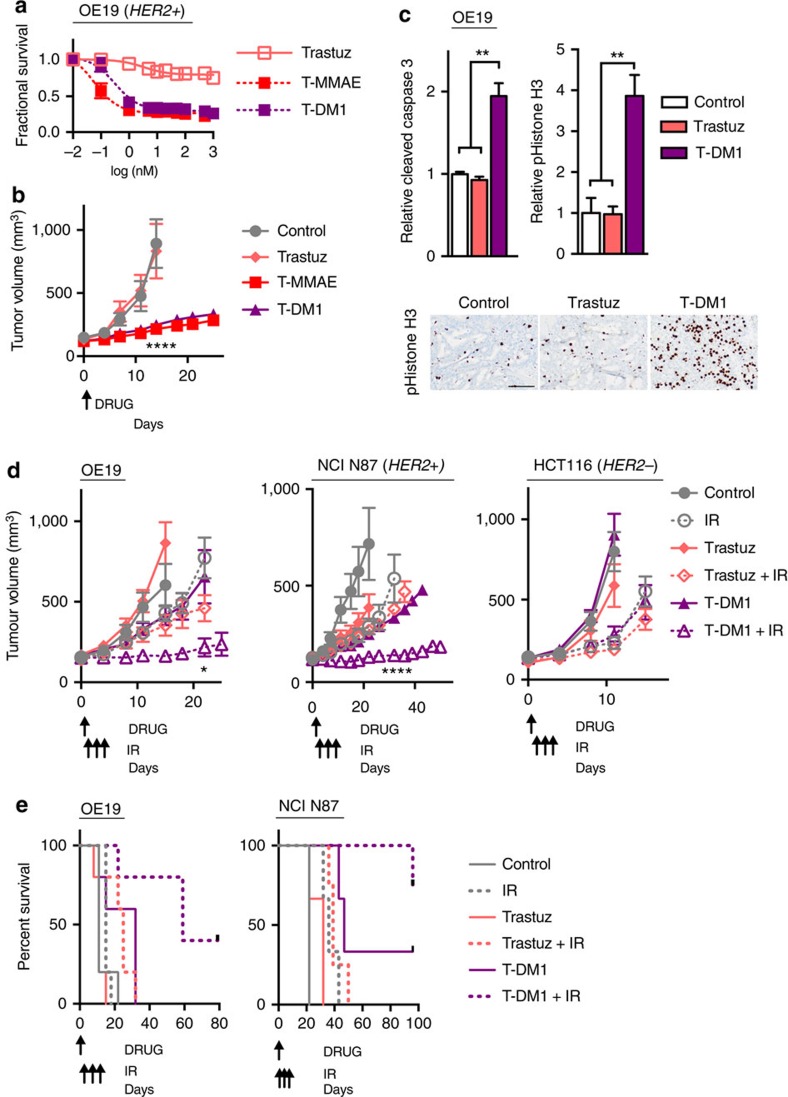
Tumour resistance to radiotherapy remains a barrier to improving cancer patient outcomes. To overcome radioresistance, certain drugs have been found to sensitize cells to ionizing radiation (IR). In theory, more potent radiosensitizing drugs should increase tumour kill and improve patient outcomes. In practice, clinical utility of potent radiosensitizing drugs is curtailed by off-target side effects. Here we report potent anti-tubulin drugs conjugated to anti-ErbB antibodies selectively radiosensitize to tumours based on surface receptor expression. While two classes of potent anti-tubulins, auristatins and maytansinoids, indiscriminately radiosensitize tumour cells, conjugating these potent anti-tubulins to anti-ErbB antibodies restrict their radiosensitizing capacity. Of translational significance, we report that a clinically used maytansinoid ADC, ado-trastuzumab emtansine (T-DM1), with IR prolongs tumour control in target expressing HER2+ tumours but not target negative tumours. In contrast to ErbB signal inhibition, our findings establish an alternative therapeutic paradigm for ErbB-based radiosensitization using antibodies to restrict radiosensitizer delivery.
Conflict of interest statement
University of California San Diego has filed patent applications based on the findings described in this manuscript (S.R.A., E.N.S., R.Y.T. and S.J.A.). The remaining authors declare no competing financial interests.
Figures




References
-
- Marur S. & Forastiere A. A. Challenges of integrating chemotherapy and targeted therapy with radiation in locally advanced head and neck squamous cell cancer. Curr. Opin. Oncol. 222, 206–211 (2010). - PubMed
-
- Laine A. M., Westover K. D. & Choy H. Radiation therapy as a backbone of treatment of locally advanced non-small cell lung cancer. Semin. Oncol. 41, 57–68 (2014). - PubMed
-
- Cohen D. J. & Leichman L. Controversies in the treatment of local and locally advanced gastric and esophageal cancers. J. Clin. Oncol. 33, 1754–1759 (2015). - PubMed
-
- Herskovic A. et al.. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N. Engl. J. Med. 326, 1593–1598 (1992). - PubMed
-
- Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet 348, 1049–1054 (1996). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
