

Managing hyperthyroidism in pregnancy: current perspectives
- PMID: 27698567
- PMCID: PMC5034921
- DOI: 10.2147/IJWH.S100987
Managing hyperthyroidism in pregnancy: current perspectives
Abstract
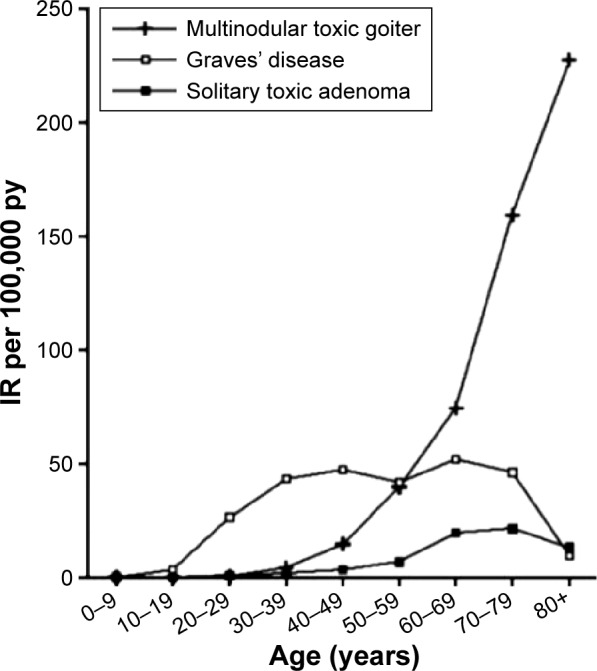
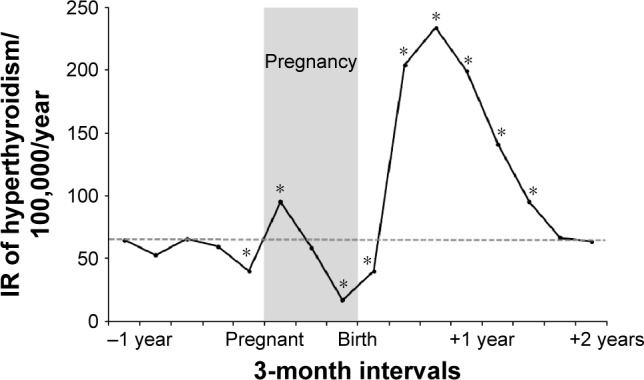
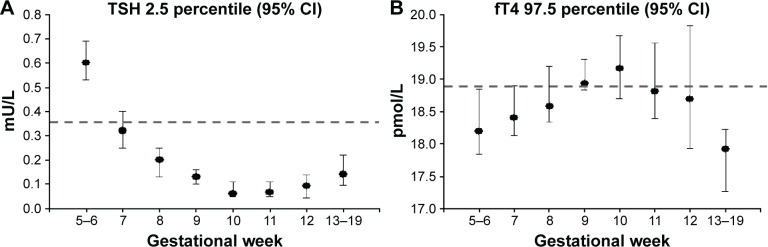
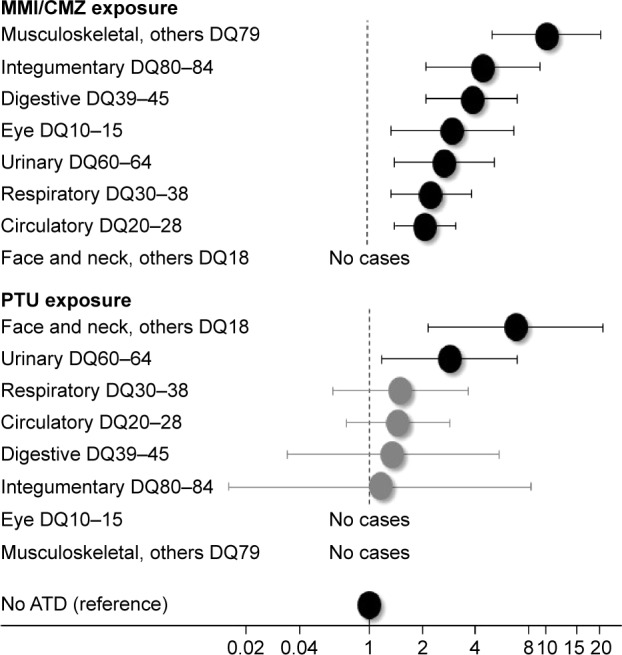
Hyperthyroidism in women who are of childbearing age is predominantly of autoimmune origin and caused by Graves' disease. The physiological changes in the maternal immune system during a pregnancy may influence the development of this and other autoimmune diseases. Furthermore, pregnancy-associated physiological changes influence the synthesis and metabolism of thyroid hormones and challenge the interpretation of thyroid function tests in pregnancy. Thyroid hormones are crucial regulators of early development and play an important role in the maintenance of a normal pregnancy and in the development of the fetus, particularly the fetal brain. Untreated or inadequately treated hyperthyroidism is associated with pregnancy complications and may even program the fetus to long-term development of disease. Thus, hyperthyroidism in pregnant women should be carefully managed and controlled, and proper management involves different medical specialties. The treatment of choice in pregnancy is antithyroid drugs (ATDs). These drugs are effective in the control of maternal hyperthyroidism, but they all cross the placenta, and so need careful management and control during the second half of pregnancy considering the risk of fetal hyper- or hypothyroidism. An important aspect in the early pregnancy is that the predominant side effect to the use of ATDs in weeks 6-10 of pregnancy is birth defects that may develop after exposure to available types of ATDs and may be severe. This review focuses on four current perspectives in the management of overt hyperthyroidism in pregnancy, including the etiology and incidence of the disease, how the diagnosis is made, the consequences of untreated or inadequately treated disease, and finally how to treat overt hyperthyroidism in pregnancy.
Keywords: Graves’ disease; antithyroid drug; fetal programming; hyperthyroidism; pregnancy; thyroid.
Figures
References
-
- Franklyn JA, Boelaert K. Thyrotoxicosis. Lancet. 2012;379(9821):1155–1166. - PubMed
-
- Bahn RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21(6):593–646. - PubMed
-
- De Groot L, Abalovich M, Alexander EK, et al. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97(8):2543–2565. - PubMed
-
- Cooper DS, Laurberg P. Hyperthyroidism in pregnancy. Lancet Diabetes Endocrinol. 2013;1(3):238–249. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
