

Breathing Better Through Bugs: Asthma and the Microbiome
- PMID: 27698615
- PMCID: PMC5045140
Breathing Better Through Bugs: Asthma and the Microbiome
Abstract
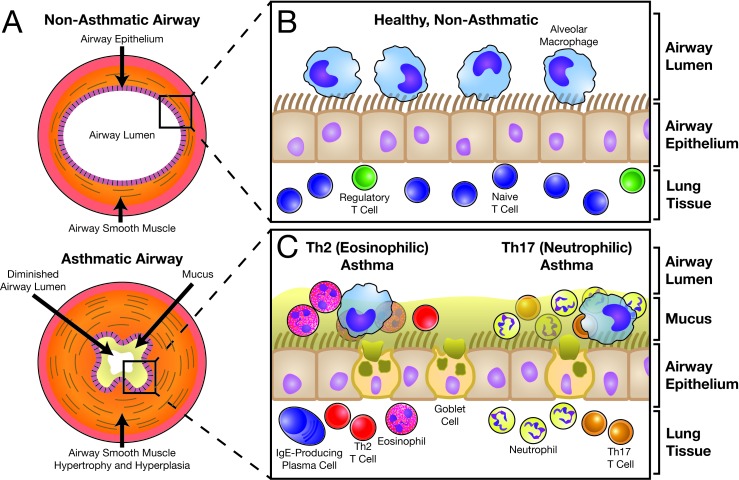
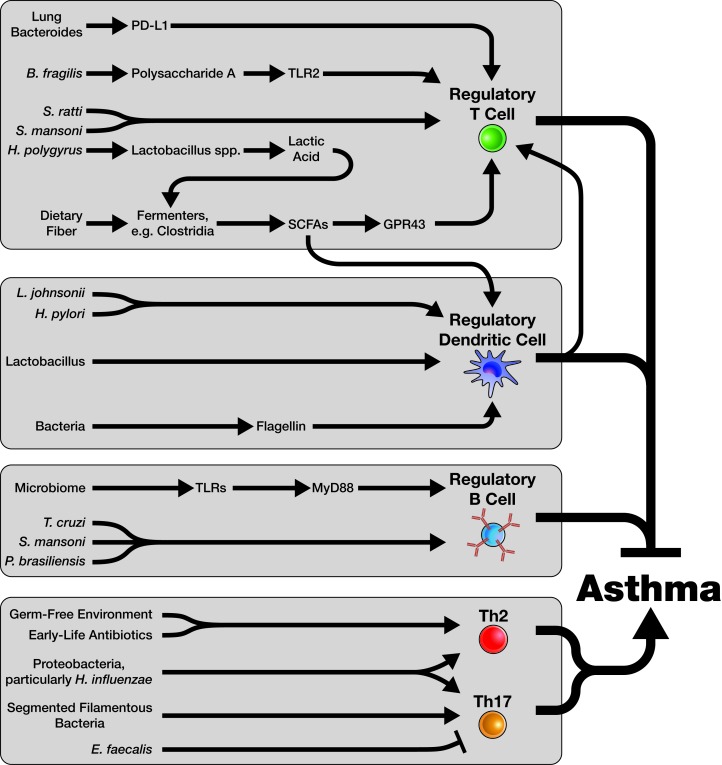
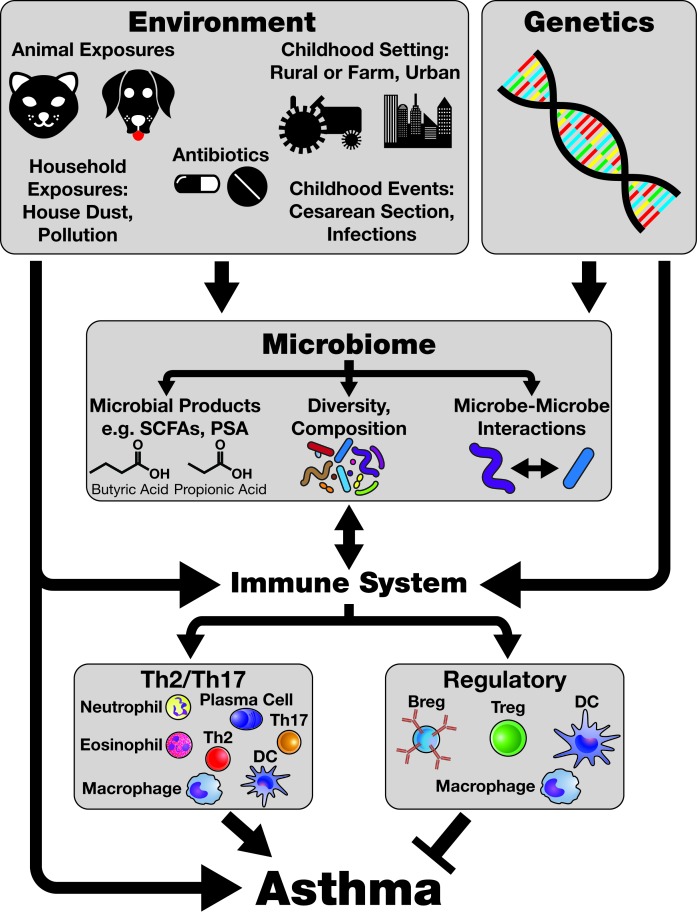
Asthma is a highly heterogeneous disease characterized by inflammation of the airways, which invokes symptoms such as wheeze, dyspnea, and chest tightness. Asthma is the product of multiple interconnected immunological processes and represents a constellation of related, but distinct, disease phenotypes. The prevalence of asthma has more than doubled since the 1980s, and efforts to understand this increase have inspired consideration of the microbiome as a key player in the pathophysiology and regulation of this disease. While recent years have seen an explosion of new research in this area, researchers are only beginning to untangle to mechanisms by which the microbiome may influence asthma. This review will focus on the relationship between the microbiome and the immune system and how this influences development of asthma. This review will also highlight evidence that may point the way toward new therapies and potential cures for this ancient respiratory foe.
Keywords: allergy; asthma; hygiene hypothesis; immune system; immunity; microbiome; microbiota.
Figures
References
-
- Postma DS, Rabe KF. The Asthma-COPD Overlap Syndrome. N Engl J Med. 2015;373(13):1241–1249. - PubMed
-
- Fanta CH. Asthma. N Engl J Med. 2009;360(10):1002–1014. - PubMed
-
- Bisgaard H, Bønnelykke K. Long-term studies of the natural history of asthma in childhood. J Allergy Clin Immunol. 2010;126(2):187–199. - PubMed
-
- Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. 2012;18(5):716–725. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases