

Diagnosing pyogenic, brucella and tuberculous spondylitis using histopathology and MRI: A retrospective study
- PMID: 27698694
- PMCID: PMC5038492
- DOI: 10.3892/etm.2016.3602
Diagnosing pyogenic, brucella and tuberculous spondylitis using histopathology and MRI: A retrospective study
Abstract
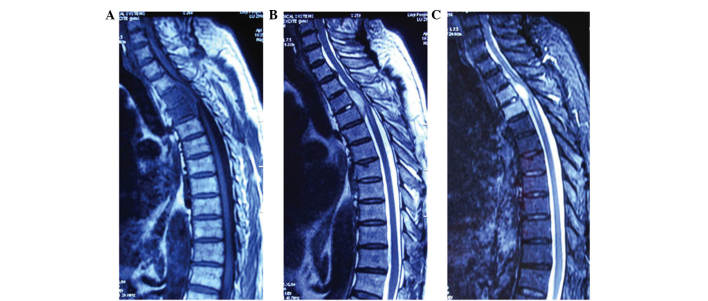
The present study examined the histopathological and magnetic resonance imaging (MRI) features of pyogenic, brucella and tuberculous spondylitis (PS, BS and TS, respectively). A total of 22 PS, 20 BS and 20 TS patients were included in the study. Histopathological examination was used to assess the lesion structure and composition, and the MRI observation identified the lesion location and signal features. The following histopathological and MRI features were identified significantly more in patients with PS than in patients with BS and TS: Predominant neutrophil infiltration, abnormal intervertebral disk signal, lesions on the ventral and lateral sides of the vertebral bodies, and thick and irregular abscess walls. The following histopathological and MRI features were identified significantly more in patients with BS than in patients with PS and TS: Predominant lymphocyte infiltration, new bone formation, epithelioid granuloma, lesions on the ventral sides of the vertebral bodies, no, or very mild, vertebral body deformation, no abnormal paraspinal soft tissue signal, no intraosseous or paraspinal abscesses, and thin and irregular abscess walls. The following histopathological and MRI features were identified significantly more in patients with TS than in patients with BS and PS: Sequestrum, Langerhans giant cells, caseous necrosis, lesions primarily in the thoracic region and on the lateral sides of the vertebral bodies, no obvious intervertebral disk damage, obvious vertebral body deformation, abnormal paraspinal soft tissue signal, intraosseous or paraspinal abscesses, and thin and smooth abscess walls. In conclusion, it can be suggested that these significant differences in histopathological and MRI features between the three different types of spondylitis may contribute towards the differential diagnosis of the diseases.
Keywords: brucella spondylitis; histopathology; magnetic resonance imaging; pyogenic spondylitis; tuberculous spondylitis.
Figures








References
-
- Wang Dali, Zhang Shiyi. Advances in treatment of acute brucellosis. Zhong Guo Gan Ran Kong Zhi Za Zhi. 2001;16:94–95. (In Chinese)
LinkOut - more resources
Full Text Sources
Other Literature Sources