

Effect of early enteral nutrition on patients with digestive tract surgery: A meta-analysis of randomized controlled trials
- PMID: 27698702
- PMCID: PMC5038219
- DOI: 10.3892/etm.2016.3559
Effect of early enteral nutrition on patients with digestive tract surgery: A meta-analysis of randomized controlled trials
Abstract
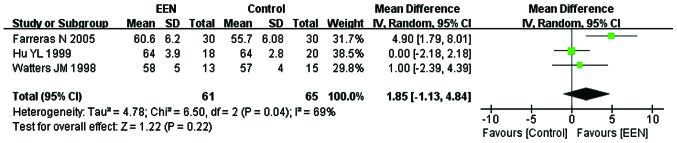
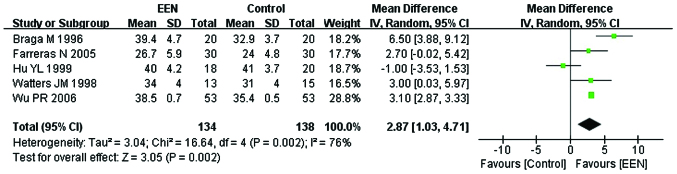
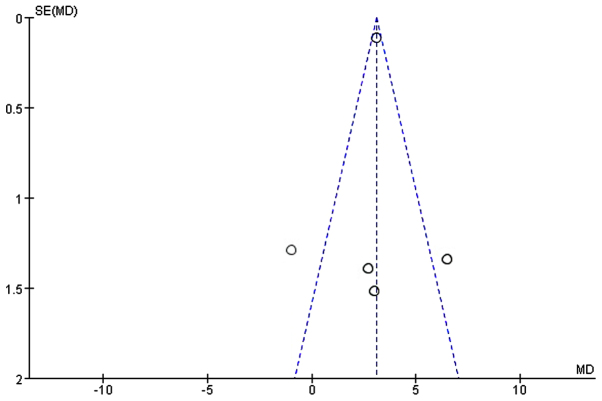
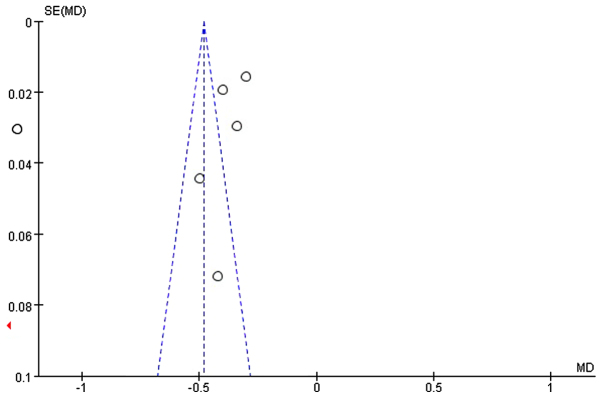
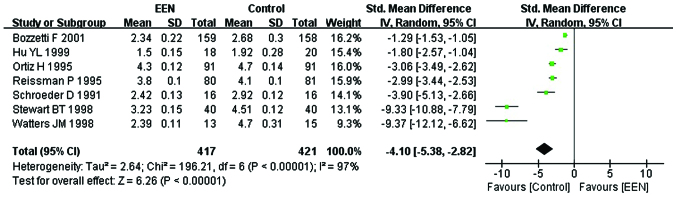
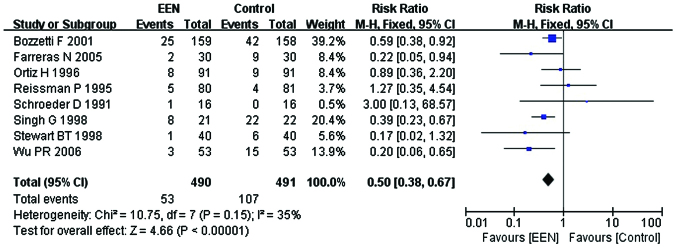
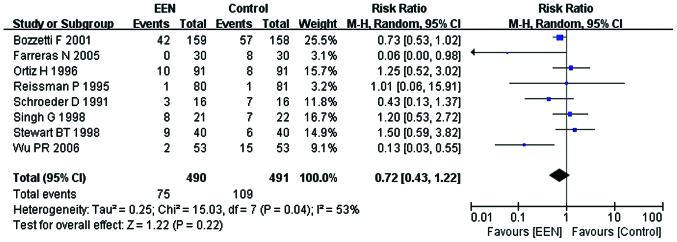
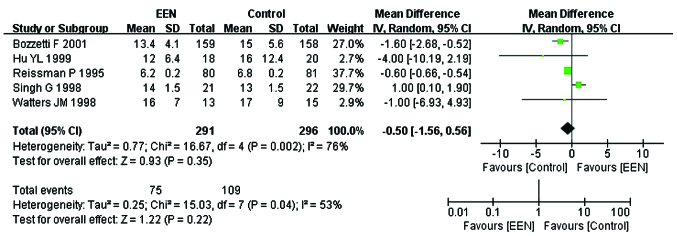
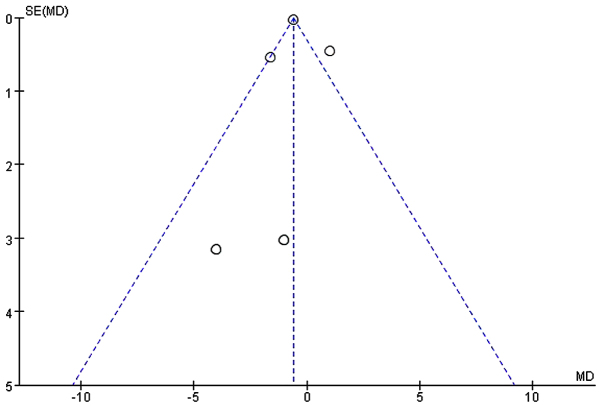
Postoperative early enteral nutrition (EEN) is useful for the effective recovery of patients that have undergone surgery. However, the feasibility and efficacy of EEN in patients with digestive tract surgery remain inconclusive. In the present meta-analysis, the PubMed, EMBASE, Web of Science, The Cochrane Library, China National Knowledge Infrastructure and VIP databases were searched to identify controlled trials of patients with and without EEN following digestive tract surgery between October, 1966 and December, 2014. Methodological quality assessment was carried out for each of the included studies. For estimation of the analysis indexes, relative risk (RR) was used as the effect size of the the categorical variable, while the weighted mean difference (MD) was used as the effect size of the continuous variable. The meta-analysis was conducted using RevMan 5.2 software. Eleven randomized controlled trials involving 1,095 patients were included in the meta-analysis. The results revealed that, EEN in patients with digestive tract surgery was more effective in decreasing the incidence of infectious [RR=0.50, 95% confidence interval (CI): 0.38, 0.67; P<0.01] and non-infectious complications (RR=0.72, 95% CI: 0.43, 1.22; P<0.05) and shortening the length of first bowel action (MD=-4.10, 95% CI: -5.38, -2.82; P<0.05). It also had a significant influence on increasing the serum albumin (MD=2.87, 95% CI: 1.03, 4.71; P<0.05) and serum prealbumin (MD=0.04, 95% CI: 0.02, 0.05; P<0.05) levels. In conclusion, the results of the study have shown that EEN in patients with digestive tract surgery improved the nutritional status, reduced the risk of postoperative complications, shortened the length of hospital stay and promoted the functional recovery of the digestive system.
Keywords: digestive tract; early enteral nutrition; meta-analysis; recovery; surgery.
Figures

References
-
- Klein S, Kinney J, Jeejeebhoy K, Alpers D, Hellerstein M, Murray M, Twomey P. Nutrition support in clinical practice: Review of published data and recommendations for future research directions. National Institutes of Health, American Society for Parenteral and Enteral Nutrition, and American Society for Clinical Nutrition. JPEN J Parenter Enteral Nutr. 1997;21:133–156. doi: 10.1177/0148607197021003133. - DOI - PubMed
-
- Chambrier C, Sztark F. Société Francophone de nutrition clinique et métabolisme (SFNEP); Société française d'anesthésie et réanimation (SFAR): French clinical guidelines on perioperative nutrition. Update of the 1994 consensus conference on perioperative artificial nutrition for elective surgery in adults. J Visc Surg. 2012;149:e325–e336. doi: 10.1016/j.jviscsurg.2012.06.006. - DOI - PubMed
-
- Pironi L, Candusso M, Biondo A, Bosco A, Castaldi P, Contaldo F, Finocchiaro E, Giannoni A, Mazzuoli S, Orlandoni P, et al. Italian Society for Parenteral and Enteral Nutrition Executive Committee: Prevalence of home artificial nutrition in Italy in 2005: A survey by the Italian Society for Parenteral and Enteral Nutrition (SINPE) Clin Nutr. 2007;26:123–132. doi: 10.1016/j.clnu.2006.07.004. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials