

FOLFIRINOX in Locally Advanced and Metastatic Pancreatic Cancer: A Single Centre Cohort Study
- PMID: 27698926
- PMCID: PMC5039370
- DOI: 10.7150/jca.16279
FOLFIRINOX in Locally Advanced and Metastatic Pancreatic Cancer: A Single Centre Cohort Study
Abstract
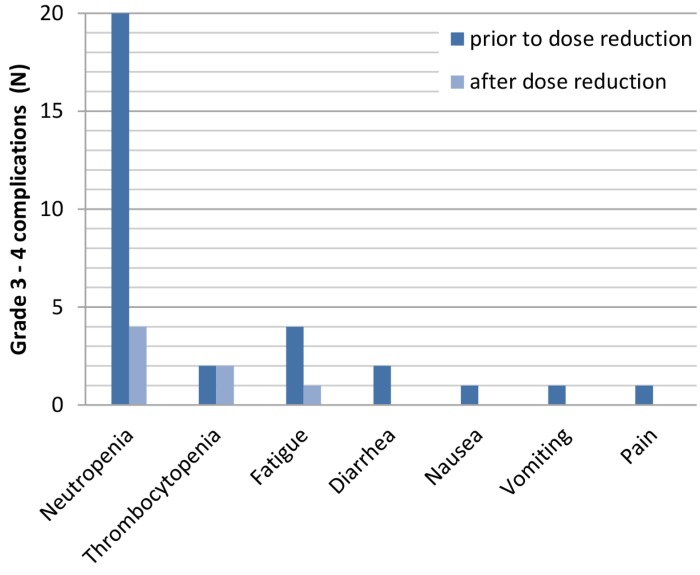
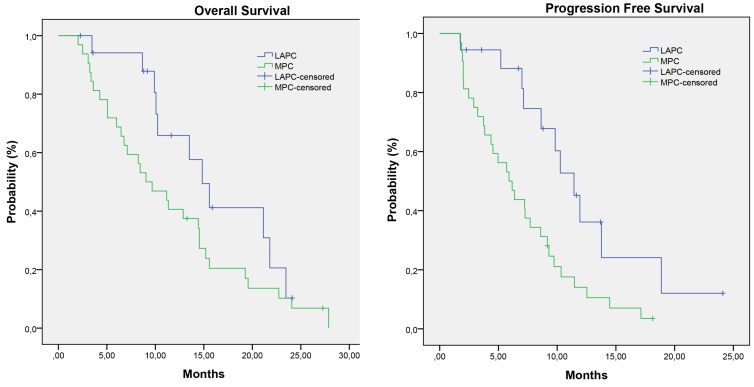
Introduction: FOLFIRINOX is emerging as new standard of care for fit patients with locally advanced pancreatic cancer (LAPC) and metastatic pancreatic cancer (MPC). However, some of the physicians are reluctant to use FOLFIRINOX due to high toxicity rates reported in earlier studies. We reviewed our experience with FOLFIRINOX in LAPC and MPC, focussing on dose adjustments, toxicity and efficacy. Methods: We reviewed all patients with LAPC or MPC treated with FOLFIRINOX in our institution between April 2011 and December 2015. Unresectability (stage III and IV) was determined by the institution's multidisciplinary team for pancreatic cancer. Results: Fifty patients (18 LAPC and 32 MPC) were enrolled, with a median age of 55 years (IQR 49-66) and WHO performance status of 0/1. FOLFIRINOX was given as first-line treatment in 82% of patients. Dose modifications were applied in 90% of patients. The median number of completed cycles was 8 (IQR 5-9). Grade 3-4 toxicity occurred in 52% and grade 5 toxicity in 2%. The response rate was 25% (12% in LAPC, 32% in MPC). Median overall survival and progression-free survival were 14.8 and 10.3 months in LAPC, and 9.0 and 5.9 months in MPC, respectively. Overall 1- and 2-year survival was 65% and 10% in LAPC and 40% and 5% in MPC. Within the LAPC group, 6 patients (33%) underwent local ablative therapy and 1 patient (6%) a resection, leading to a median survival of 21.8 months. Conclusion: FOLFIRINOX treatment with nearly routine dose modification was associated with acceptable toxicity rates, relatively high response rates and an encouraging overall survival.
Keywords: FOLFIRINOX; advanced stage; efficacy; pancreatic cancer; stage III and IV; toxicity.
Conflict of interest statement
Professor doctor HWM van Laarhoven has served as a consultant for Celgene, Lilly, and Nordic, and has received unrestricted research funding from Bayer, Celgene, GSK, Janssen Cilag, Lilly, Merck Serono, MSD, Nordic, and Roche. All of the other authors declare to have no conflict of interest or a source of funding relevant to this article.
Figures
References
-
- National Cancer Institute: Pancreatic Cancer Facts; Revised 5 February 2016. http://seer.cancer.gov/statfacts/html/pancreas.html.
-
- Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J. et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013 Apr;49(6):1374–403. - PubMed
-
- Oncoline: Pancreatic cancer; Revised 5 February 2016. http://www.oncoline.nl/pancreascarcinoom.
-
- Burris HA 3rd, Moore MJ, Andersen J. et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15:2403–13. - PubMed
-
- Conroy T, Desseigne F, Ychou M. et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
