

Reversal of Vascular Calcification and Aneurysms in a Rat Model Using Dual Targeted Therapy with EDTA- and PGG-Loaded Nanoparticles
- PMID: 27698934
- PMCID: PMC5039337
- DOI: 10.7150/thno.16547
Reversal of Vascular Calcification and Aneurysms in a Rat Model Using Dual Targeted Therapy with EDTA- and PGG-Loaded Nanoparticles
Abstract
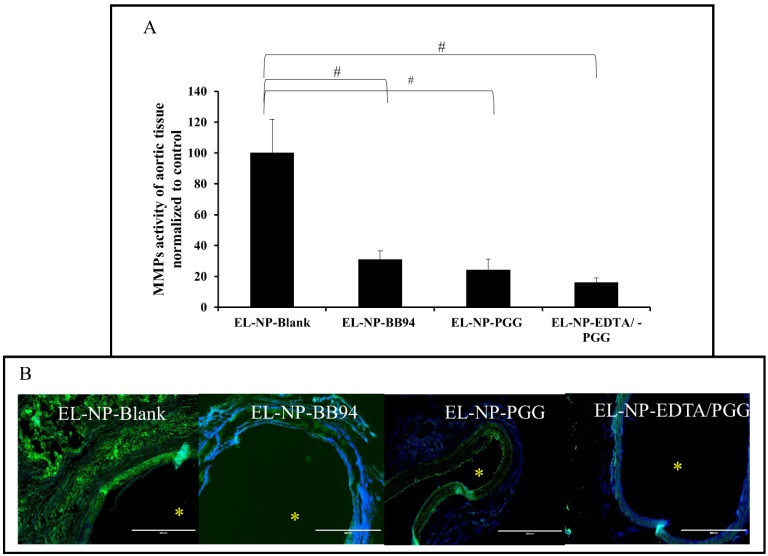
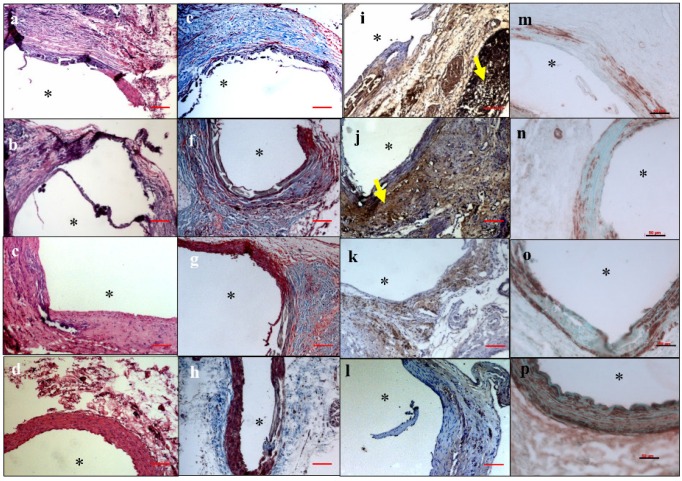
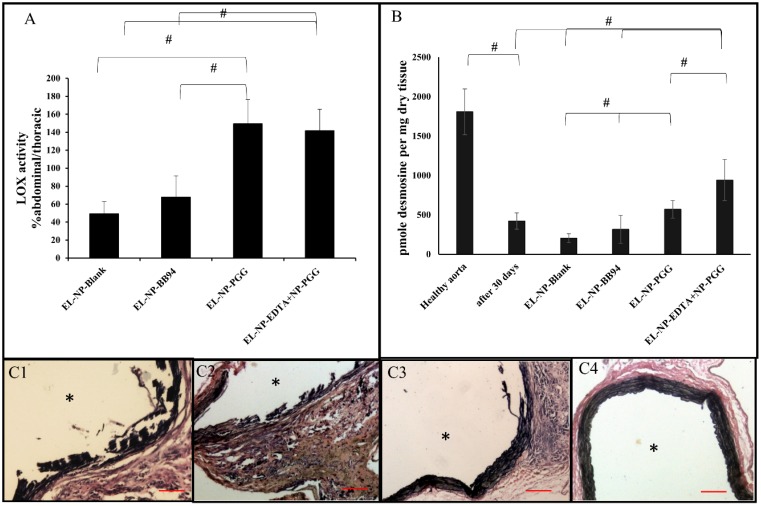
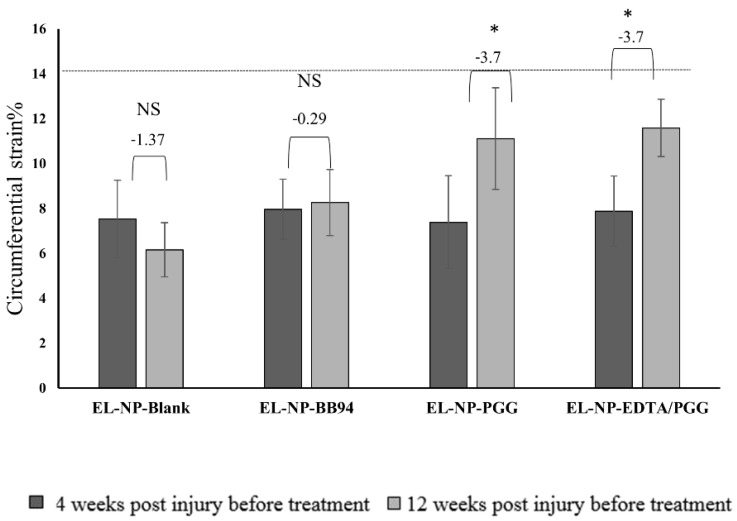
Degeneration of elastic lamina and vascular calcification are common features of vascular pathology such as aortic aneurysms. We tested whether dual therapy with targeted nanoparticles (NPs) can remove mineral deposits (by delivery of a chelating agent, ethylene diamine tetraacetic acid (EDTA)) and restore elastic lamina (by delivery of a polyphenol, pentagalloyl glucose (PGG)) to reverse moderate aneurysm development. EDTA followed by PGG NP delivery led to reduction in macrophage recruitment, matrix metalloproteinase (MMP) activity, elastin degradation and calcification in the aorta as compared to delivery of control blank NPs. Such dual therapy restored vascular elastic lamina and improved vascular function as observed by improvement in circumferential strain. Therefore, dual targeted therapy may be an attractive option to remove mineral deposits and restore healthy arterial structures in moderately developed aneurysms.
Keywords: AAA; PGG.; calcification; chelation therapy; elastin.
Conflict of interest statement
The authors have declared that no competing interest exists.
Figures
Similar articles
-
Nanoparticle-based targeted delivery of pentagalloyl glucose reverses elastase-induced abdominal aortic aneurysm and restores aorta to the healthy state in mice.PLoS One. 2020 Mar 27;15(3):e0227165. doi: 10.1371/journal.pone.0227165. eCollection 2020. PLoS One. 2020. PMID: 32218565 Free PMC article.
-
Systemic Delivery of Nanoparticles Loaded with Pentagalloyl Glucose Protects Elastic Lamina and Prevents Abdominal Aortic Aneurysm in Rats.J Cardiovasc Transl Res. 2016 Dec;9(5-6):445-455. doi: 10.1007/s12265-016-9709-x. Epub 2016 Aug 19. J Cardiovasc Transl Res. 2016. PMID: 27542007
-
Site-specific chelation therapy with EDTA-loaded albumin nanoparticles reverses arterial calcification in a rat model of chronic kidney disease.Sci Rep. 2019 Feb 22;9(1):2629. doi: 10.1038/s41598-019-39639-8. Sci Rep. 2019. PMID: 30796300 Free PMC article.
-
Pentagalloyl Glucose and Its Functional Role in Vascular Health: Biomechanics and Drug-Delivery Characteristics.Ann Biomed Eng. 2019 Jan;47(1):39-59. doi: 10.1007/s10439-018-02145-5. Epub 2018 Oct 8. Ann Biomed Eng. 2019. PMID: 30298373 Free PMC article. Review.
-
Vascular diseases: aortitis, aortic aneurysms, and vascular calcification.Cardiovasc Pathol. 2016 Sep-Oct;25(5):432-41. doi: 10.1016/j.carpath.2016.07.002. Epub 2016 Jul 14. Cardiovasc Pathol. 2016. PMID: 27526100 Review.
Cited by
-
Nano-Biomaterials for the Delivery of Therapeutic and Monitoring Cues for Aortic Diseases.Front Bioeng Biotechnol. 2020 Nov 5;8:583879. doi: 10.3389/fbioe.2020.583879. eCollection 2020. Front Bioeng Biotechnol. 2020. PMID: 33224934 Free PMC article. Review.
-
Pentagalloyl glucose from Schinus terebinthifolia inhibits growth of carbapenem-resistant Acinetobacter baumannii.Sci Rep. 2020 Sep 18;10(1):15340. doi: 10.1038/s41598-020-72331-w. Sci Rep. 2020. PMID: 32948818 Free PMC article.
-
EDTA-Modified 17β-Estradiol-Laden Upconversion Nanocomposite for Bone-Targeted Hormone Replacement Therapy for Osteoporosis.Theranostics. 2020 Feb 10;10(7):3281-3292. doi: 10.7150/thno.37599. eCollection 2020. Theranostics. 2020. PMID: 32194868 Free PMC article.
-
Nanoparticle-based targeted delivery of pentagalloyl glucose reverses elastase-induced abdominal aortic aneurysm and restores aorta to the healthy state in mice.PLoS One. 2020 Mar 27;15(3):e0227165. doi: 10.1371/journal.pone.0227165. eCollection 2020. PLoS One. 2020. PMID: 32218565 Free PMC article.
-
Matrix Metalloproteinase in Abdominal Aortic Aneurysm and Aortic Dissection.Pharmaceuticals (Basel). 2019 Aug 6;12(3):118. doi: 10.3390/ph12030118. Pharmaceuticals (Basel). 2019. PMID: 31390798 Free PMC article. Review.
References
-
- Kent KC. Abdominal aortic aneurysms. N Engl J Med. 2014;371:2101–8. - PubMed
-
- Assar AN, Zarins C. Ruptured abdominal aortic aneurysm: a surgical emergency with many clinical presentations. Postgraduate medical journal. 2009;85:268–73. - PubMed
-
- Ishizaka N, Sohmiya K, Miyamura M, Umeda T, Tsuji M, Katsumata T. et al. Infected aortic aneurysm and inflammatory aortic aneurysm—in search of an optimal differential diagnosis. Journal of cardiology. 2012;59:123–31. - PubMed
-
- Mäyränpää MI, Trosien JA, Fontaine V, Folkesson M, Kazi M, Eriksson P. et al. Mast cells associate with neovessels in the media and adventitia of abdominal aortic aneurysms. Journal of vascular surgery. 2009;50:388–95. - PubMed
-
- Li Z-Y, Jean U, Tang TY, Soh E, See TC, Gillard JH. Impact of calcification and intraluminal thrombus on the computed wall stresses of abdominal aortic aneurysm. Journal of vascular surgery. 2008;47:928–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
