

The rate of brain death and organ donation in patients resuscitated from cardiac arrest: a systematic review and meta-analysis
- PMID: 27699457
- PMCID: PMC5069310
- DOI: 10.1007/s00134-016-4549-3
The rate of brain death and organ donation in patients resuscitated from cardiac arrest: a systematic review and meta-analysis
Abstract
Background: The occurrence of brain death in patients with hypoxic-ischaemic brain injury after resuscitation from cardiac arrest creates opportunities for organ donation. However, its prevalence is currently unknown.
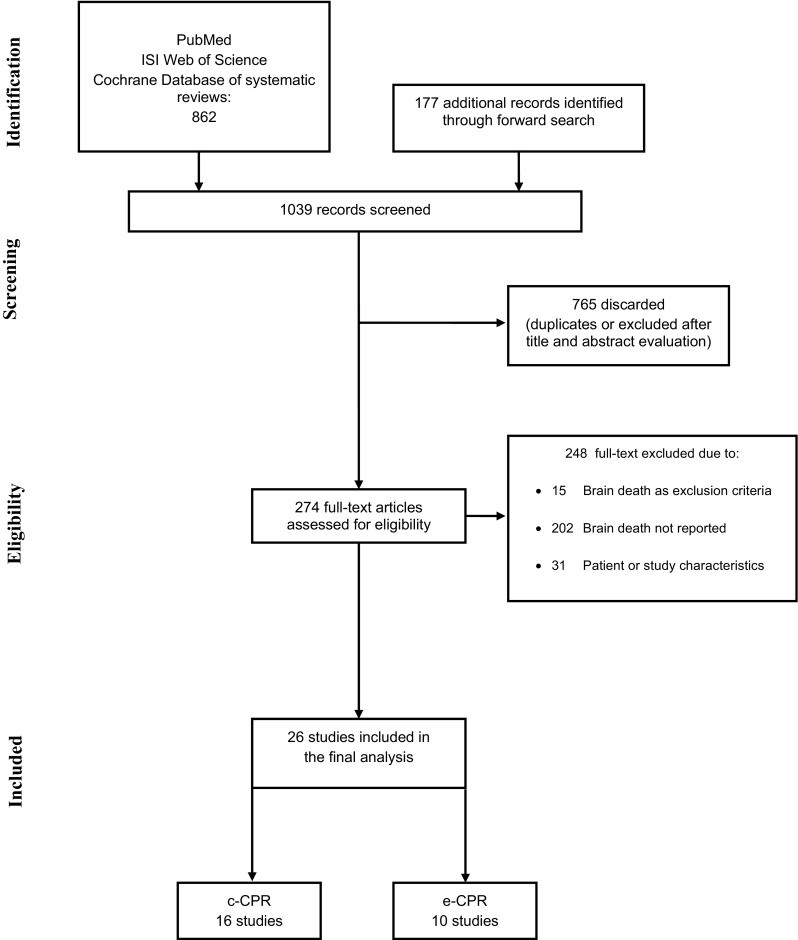
Methods: Systematic review. MEDLINE via PubMed, ISI Web of Science and the Cochrane Database of Systematic Reviews were searched for eligible studies (2002-2016). The prevalence of brain death in adult patients resuscitated from cardiac arrest and the rate of organ donation among brain dead patients were summarised using a random effect model with double-arcsine transformation. The quality of evidence (QOE) was evaluated according to the GRADE guidelines.
Results: 26 studies [16 on conventional cardiopulmonary resuscitation (c-CPR), 10 on extracorporeal CPR (e-CPR)] included a total of 23,388 patients, 1830 of whom developed brain death at a mean time of 3.2 ± 0.4 days after recovery of circulation. The overall prevalence of brain death among patients who died before hospital discharge was 12.6 [10.2-15.2] %. Prevalence was significantly higher in e-CPR vs. c-CPR patients (27.9 [19.7-36.6] vs. 8.3 [6.5-10.4] %; p < 0.0001). The overall rate of organ donation among brain dead patients was 41.8 [20.2-51.0] % (9/26 studies, 1264 patients; range 0-100 %). The QOE was very low for both outcomes.
Conclusions: In patients with hypoxic-ischaemic brain injury following CPR, more than 10 % of deaths were due to brain death. More than 40 % of brain-dead patients could donate organs. Patients who are unconscious after resuscitation from cardiac arrest, especially when resuscitated using e-CPR, should be carefully screened for signs of brain death.
Keywords: Anoxia-ischemia, brain; Brain death; Cardiac arrest; Organ donation.
Conflict of interest statement
Compliance with ethical standards Conflicts of interest On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures

Comment in
-
Authors' response: CPR and brain death: confounders, clearance, caution.Intensive Care Med. 2017 Feb;43(2):286-287. doi: 10.1007/s00134-016-4632-9. Epub 2016 Nov 28. Intensive Care Med. 2017. PMID: 27896380 No abstract available.
-
CPR and brain death: confounders, clearance, caution.Intensive Care Med. 2017 Feb;43(2):284-285. doi: 10.1007/s00134-016-4625-8. Epub 2016 Nov 28. Intensive Care Med. 2017. PMID: 27896381 No abstract available.
References
-
- Lemiale V, Dumas F, Mongardon N, Giovanetti O, Charpentier J, Chiche JD, Carli P, Mira JP, Nolan J, Cariou A. Intensive care unit mortality after cardiac arrest: the relative contribution of shock and brain injury in a large cohort. Intensive Care Med. 2013;39:1972–1980. doi: 10.1007/s00134-013-3043-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
