

Outpatient administration of BEAM conditioning prior to autologous stem cell transplantation for lymphoma is safe, feasible, and cost-effective
- PMID: 27699999
- PMCID: PMC5119960
- DOI: 10.1002/cam4.879
Outpatient administration of BEAM conditioning prior to autologous stem cell transplantation for lymphoma is safe, feasible, and cost-effective
Abstract
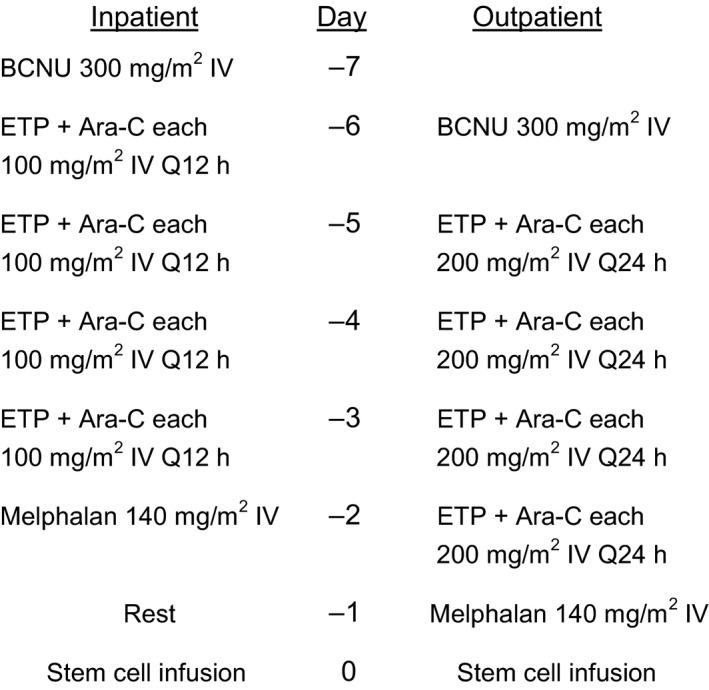
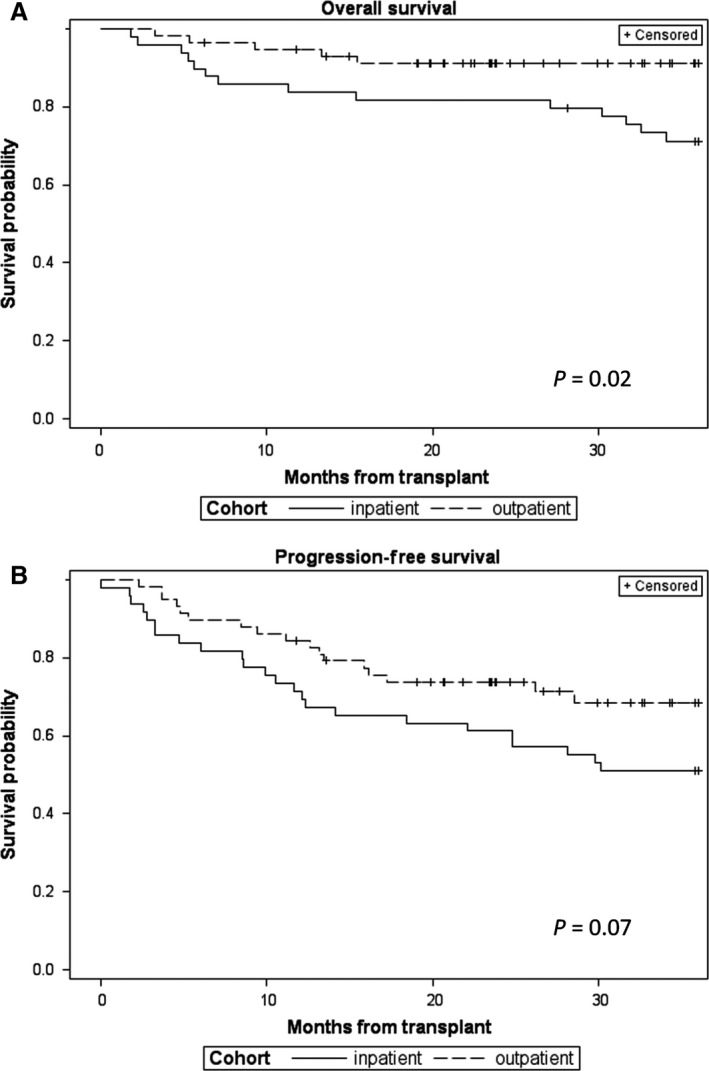
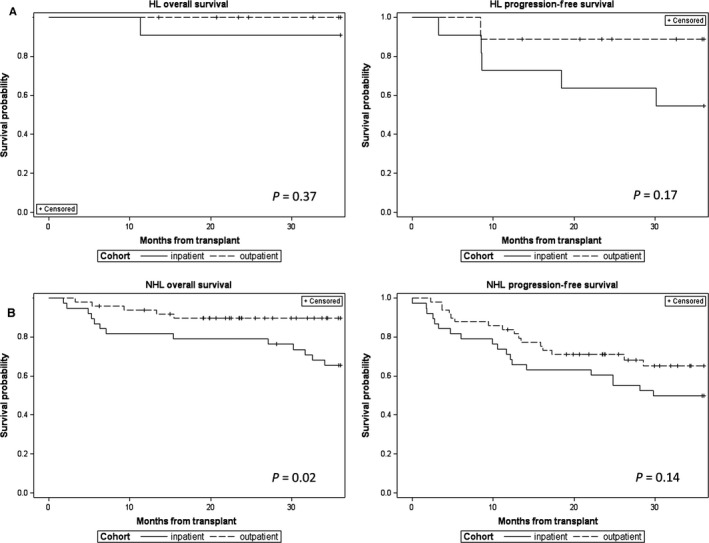
High-dose BEAM chemotherapy (BCNU, etoposide, Ara-C, and melphalan) followed by autologous hematopoietic stem cell transplantation is frequently used as consolidative therapy for patients with recurrent or refractory Hodgkin or non-Hodgkin lymphoma. The BEAM regimen has traditionally been administered over 6 days in the hospital, with patients remaining hospitalized until hematologic recovery and clinical stability. In an effort to reduce the length of hospitalization for these patients, our institution has transitioned from inpatient (IP) to outpatient (OP) administration of BEAM conditioning. Here, we report the results of an analysis of the feasibility, cost, complications, and outcomes for the initial group of patients who received OP BEAM compared to a prior cohort of patients who received IP BEAM. Patient and disease characteristics were comparable for the two cohorts, as were engraftment kinetics. Length of hospital stay was reduced by 6 days for the OP cohort (P < 0.001), resulting in a cost savings of more than $17,000 per patient. Fewer complications occurred in the OP cohort, including severe enteritis (P = 0.01), organ toxicities (P = 0.01), and infections (P = 0.04). Overall survival rate up to 3 years posttransplant was better for the OP cohort (P = 0.02), likely due to differences in posttransplant therapies. We conclude that OP administration of BEAM conditioning is safe and may offer significant advantages, including decreased length of hospitalization, reduced costs, decreased risks for severe toxicities and infectious complications, and likely improvement in patient satisfaction and quality of life.
Keywords: Complications; conditioning chemotherapy; cost; stem cell transplantation.
© 2016 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Figures
References
-
- Linch, D. C. , Winfield D., Goldstone A. H., Moir D., Hancock B., McMillan A., et. al. 1993. Dose intensification with autologous bone‐marrow transplantation in relapsed and resistant Hodgkin's disease: results of a BNLI randomized trial. Lancet 341:1051–1054. - PubMed
-
- Philip, T. , Guglielmi C., Hagenbeek A., Somers R., Van der Lelie H., Bron D., et al. 1995. Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy‐sensitive non‐Hodgkin's lymphoma. N. Engl. J. Med. 333:1540–1545. - PubMed
-
- Hahn, T. , Wolff S. N., Czuczman M., Fisher R. I., Lazarus H. M., Vose J. et al. 2001. The role of cytotoxic therapy with hematopoietic stem cell transplantation in the therapy of diffuse large cell B‐cell non‐Hodgkin's lymphoma: an evidence‐based review. Biol. Blood Marrow Transplant. 7:308–331. - PubMed
-
- Schmitz, N. , Pfistner B., Sextro M., Sieber M., Carella A. M., Haenel M., et al. 2002. Aggressive conventional chemotherapy compared with high‐dose chemotherapy with autologous haemopoietic stem‐cell transplantation for relapsed chemosensitive Hodgkin's disease: a randomized trial. Lancet 359:2065–2071. - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
