

Factors associated with recurrence and survival length following relapse in patients with neuroblastoma
- PMID: 27701387
- PMCID: PMC5117794
- DOI: 10.1038/bjc.2016.302
Factors associated with recurrence and survival length following relapse in patients with neuroblastoma
Abstract
Background: Despite therapeutic advances, survival following relapse for neuroblastoma patients remains poor. We investigated clinical and biological factors associated with length of progression-free and overall survival following relapse in UK neuroblastoma patients.
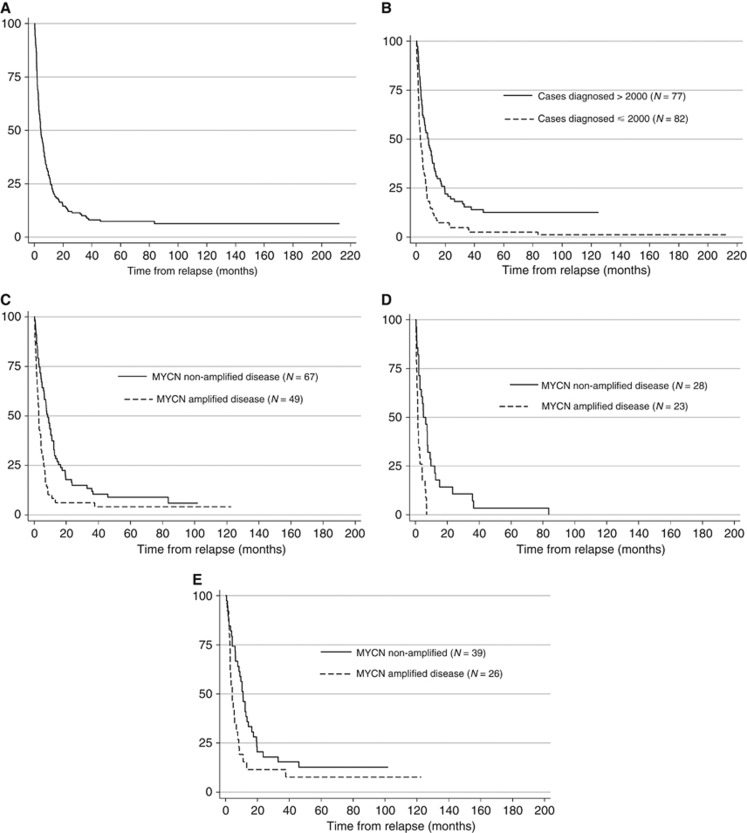
Methods: All cases of relapsed neuroblastoma, diagnosed during 1990-2010, were identified from four Paediatric Oncology principal treatment centres. Kaplan-Meier and Cox regression analyses were used to calculate post-relapse overall survival (PROS), post-relapse progression-free survival (PRPFS) between relapse and further progression, and to investigate influencing factors.
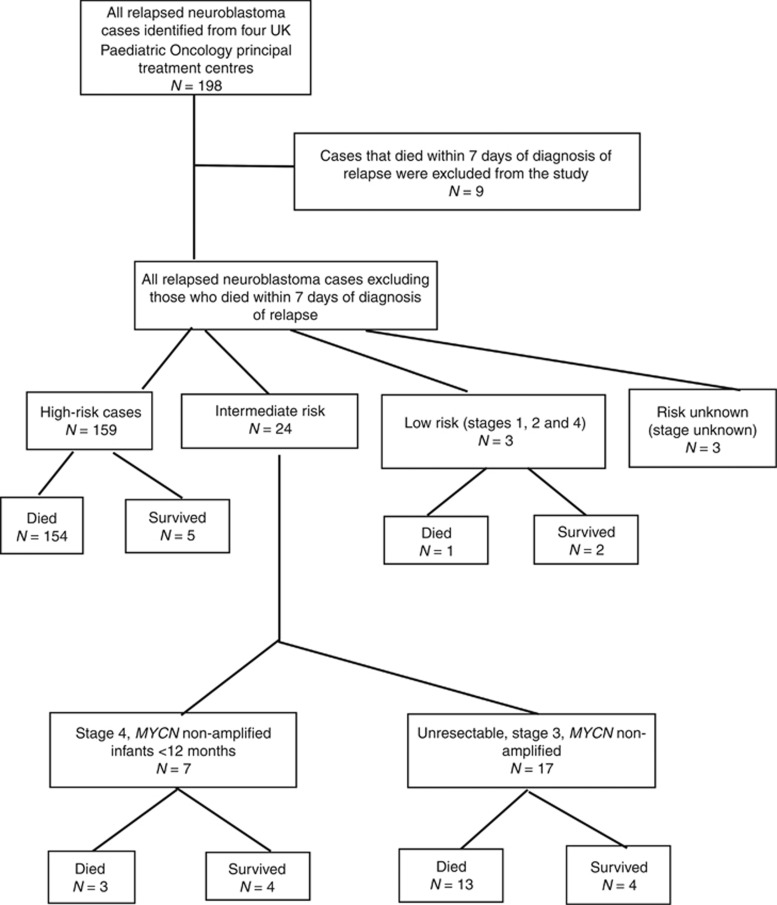
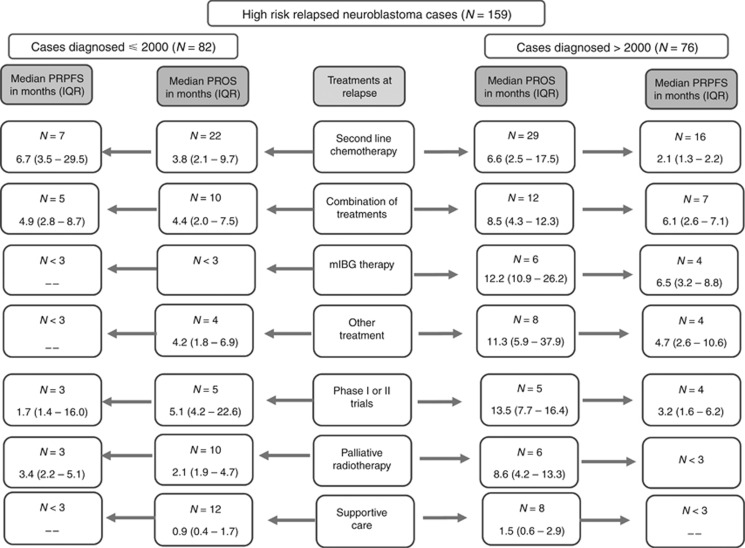
Results: One hundred eighty-nine cases were identified from case notes, 159 (84.0%) high risk and 17 (9.0%), unresectable, MYCN non-amplified (non-MNA) intermediate risk (IR). For high-risk patients diagnosed >2000, median PROS was 8.4 months (interquartile range (IQR)=3.0-17.4) and median PRPFS was 4.7 months (IQR=2.1-7.1). For IR, unresectable non-MNA patients, median PROS was 11.8 months (IQR 9.0-51.6) and 5-year PROS was 24% (95% CI 7-45%). MYCN amplified (MNA) disease and bone marrow metastases at diagnosis were independently associated with worse PROS for high-risk cases. Eighty percent of high-risk relapses occurred within 2 years of diagnosis compared with 50% of unresectable non-MNA IR disease.
Conclusions: Patients with relapsed HR neuroblastomas should be treatment stratified according to MYCN status and PRPFS should be the primary endpoint in early phase clinical trials. The failure to salvage the majority of IR neuroblastoma is concerning, supporting investigation of intensification of upfront treatment regimens in this group to determine whether their use would diminish likelihood of relapse.
Conflict of interest statement
Dr Lucas Moreno discloses the following activities: consultancy/advisory board participation for Novartis, AstraZeneca, RocheGenentech, Mundipharma and Bayer. The remaining authors declare no conflict of interest.
Figures
References
-
- Attiyeh EF, London WB, Mossé YP, Wang Q, Winter C, Khazi D, McGrady PW, Seeger RC, Look AT, Shimada H, Brodeur GM, Cohn SL, Matthay KK, Maris JM Children's Oncology Group (2005) Chromosome 1p and 11q deletions and outcome in neuroblastoma. N Engl J Med 353: 2243–2253. - PubMed
-
- Bagatell R, Rumcheva P, London WB, Cohn SL, Look AT, Brodeur GM, Frantz C, Joshi V, Thorner P, Rao PV, Castleberry R, Bowman LC (2005) Outcomes of children with intermediate-risk neuroblastoma after treatment stratified by MYCN status and tumor cell ploidy. J Clin Oncol 23: 8819–8827. - PubMed
-
- Baker DL, Schmidt ML, Cohn SL, Maris JM, London WB, Buxton A, Stram D, Castleberry RP, Shimada H, Sandler A, Shamberger RC, Look AT, Reynolds CP, Seeger RC, Matthay KK Children's Oncology Group (2010) Outcome after reduced chemotherapy for intermediate-risk neuroblastoma. N Engl J Med 363: 1313–1323. - PMC - PubMed
-
- Birch JM (1988) Manchester children's tumour registry 1954–1970 and 1971–1983. In International Incidence of Childhood Cancer DM Parkin, CA Stiller, GJ Draper, CA Bieber, B Terracini, JL Young, (eds). 299–304. IARC: Lyon.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
