

Association Between Therapeutic Hypothermia and Survival After In-Hospital Cardiac Arrest
- PMID: 27701659
- PMCID: PMC5486217
- DOI: 10.1001/jama.2016.14380
Association Between Therapeutic Hypothermia and Survival After In-Hospital Cardiac Arrest
Abstract
Importance: Therapeutic hypothermia is used for patients following both out-of-hospital and in-hospital cardiac arrest. However, randomized trials on its efficacy for the in-hospital setting do not exist, and comparative effectiveness data are limited.
Objective: To evaluate the association between therapeutic hypothermia and survival after in-hospital cardiac arrest.
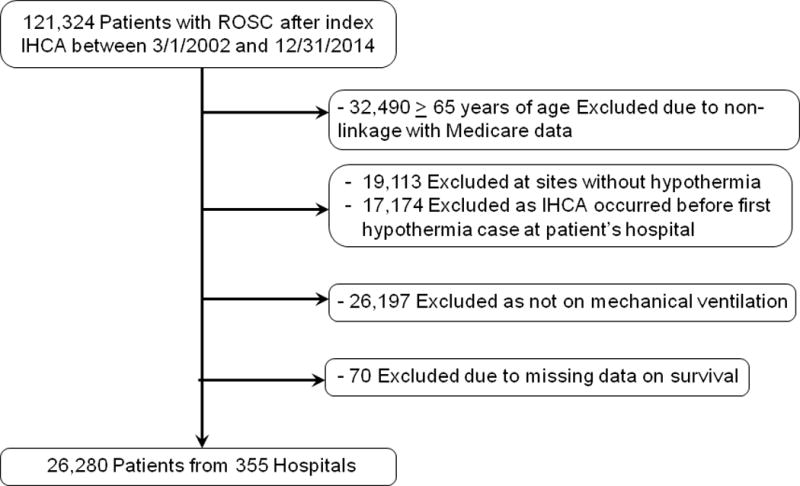
Design, setting, and patients: In this cohort study, within the national Get With the Guidelines-Resuscitation registry, 26 183 patients successfully resuscitated from an in-hospital cardiac arrest between March 1, 2002, and December 31, 2014, and either treated or not treated with hypothermia at 355 US hospitals were identified. Follow-up ended February 4, 2015.
Exposure: Induction of therapeutic hypothermia.
Main outcomes and measures: The primary outcome was survival to hospital discharge. The secondary outcome was favorable neurological survival, defined as a Cerebral Performance Category score of 1 or 2 (ie, without severe neurological disability). Comparisons were performed using a matched propensity score analysis and examined for all cardiac arrests and separately for nonshockable (asystole and pulseless electrical activity) and shockable (ventricular fibrillation and pulseless ventricular tachycardia) cardiac arrests.
Results: Overall, 1568 of 26 183 patients with in-hospital cardiac arrest (6.0%) were treated with therapeutic hypothermia; 1524 of these patients (mean [SD] age, 61.6 [16.2] years; 58.5% male) were matched by propensity score to 3714 non-hypothermia-treated patients (mean [SD] age, 62.2 [17.5] years; 57.1% male). After adjustment, therapeutic hypothermia was associated with lower in-hospital survival (27.4% vs 29.2%; relative risk [RR], 0.88 [95% CI, 0.80 to 0.97]; risk difference, -3.6% [95% CI, -6.3% to -0.9%]; P = .01), and this association was similar (interaction P = .74) for nonshockable cardiac arrest rhythms (22.2% vs 24.5%; RR, 0.87 [95% CI, 0.76 to 0.99]; risk difference, -3.2% [95% CI, -6.2% to -0.3%]) and shockable cardiac arrest rhythms (41.3% vs 44.1%; RR, 0.90 [95% CI, 0.77 to 1.05]; risk difference, -4.6% [95% CI, -10.9% to 1.7%]). Therapeutic hypothermia was also associated with lower rates of favorable neurological survival for the overall cohort (hypothermia-treated group, 17.0% [246 of 1443 patients]; non-hypothermia-treated group, 20.5% [725 of 3529 patients]; RR, 0.79 [95% CI, 0.69 to 0.90]; risk difference, -4.4% [95% CI, -6.8% to -2.0%]; P < .001) and for both rhythm types (interaction P = .88).
Conclusions and relevance: Among patients with in-hospital cardiac arrest, use of therapeutic hypothermia compared with usual care was associated with a lower likelihood of survival to hospital discharge and a lower likelihood of favorable neurological survival. These observational findings warrant a randomized clinical trial to assess efficacy of therapeutic hypothermia for in-hospital cardiac arrest.
Conflict of interest statement
Dr. Chan has served as a consultant for the American Heart Association. None of the other authors has any conflicts of interest or financial interests to disclose.
GWTG-Resuscitation is sponsored by the American Heart Association, which had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The manuscript was reviewed and approved by the GWTG-Resuscitation research and publications committee prior to journal submission.
Figures
Comment in
-
Therapeutic hypothermia has no benefit for in-hospital cardiac arrest, study finds.BMJ. 2016 Oct 5;355:i5409. doi: 10.1136/bmj.i5409. BMJ. 2016. PMID: 27758780 No abstract available.
-
Therapeutic Hypothermia After Cardiac Arrest.JAMA. 2017 Feb 14;317(6):644. doi: 10.1001/jama.2016.19826. JAMA. 2017. PMID: 28196245 No abstract available.
-
Therapeutic Hypothermia After Cardiac Arrest.JAMA. 2017 Feb 14;317(6):644. doi: 10.1001/jama.2016.19829. JAMA. 2017. PMID: 28196246 No abstract available.
-
Therapeutic Hypothermia Doesn't Improve Survival or Neurologic Outcomes After In-Hospital Cardiac Arrest.Am J Nurs. 2017 Mar;117(3):70. doi: 10.1097/01.NAJ.0000513296.34569.d2. Am J Nurs. 2017. PMID: 28230700 No abstract available.
References
-
- Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
-
- Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Kory P, Fukunaga M, Mathew JP, et al. Outcomes of mild therapeutic hypothermia after in-hospital cardiac arrest. Neurocrit Care. 2012;16:406–412. - PubMed
-
- Nichol G, Huszti E, Kim F, et al. Does induction of hypothermia improve outcomes after in-hospital cardiac arrest? Resuscitation. 2013;84:620–625. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
