

Cost-effectiveness analysis of online hemodiafiltration versus high-flux hemodialysis
- PMID: 27703388
- PMCID: PMC5036827
- DOI: 10.2147/CEOR.S109649
Cost-effectiveness analysis of online hemodiafiltration versus high-flux hemodialysis
Abstract
Background: Clinical studies suggest that hemodiafiltration (HDF) may lead to better clinical outcomes than high-flux hemodialysis (HF-HD), but concerns have been raised about the cost-effectiveness of HDF versus HF-HD. Aim of this study was to investigate whether clinical benefits, in terms of longer survival and better health-related quality of life, are worth the possibly higher costs of HDF compared to HF-HD.
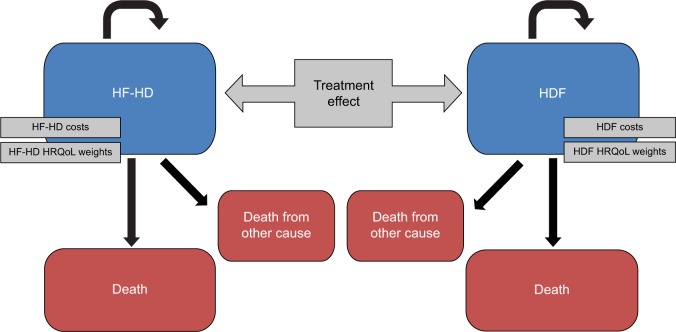
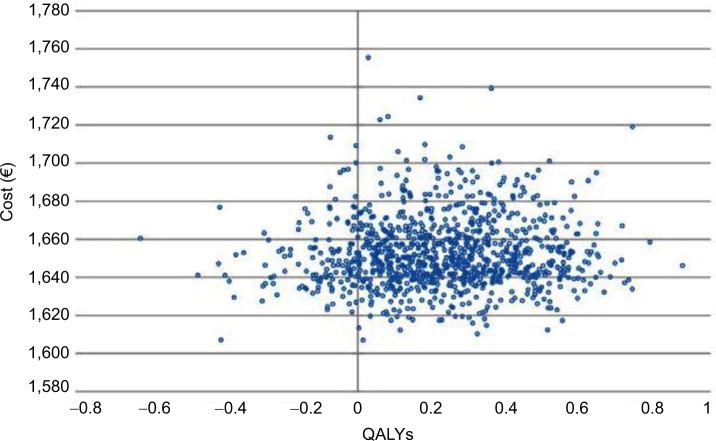
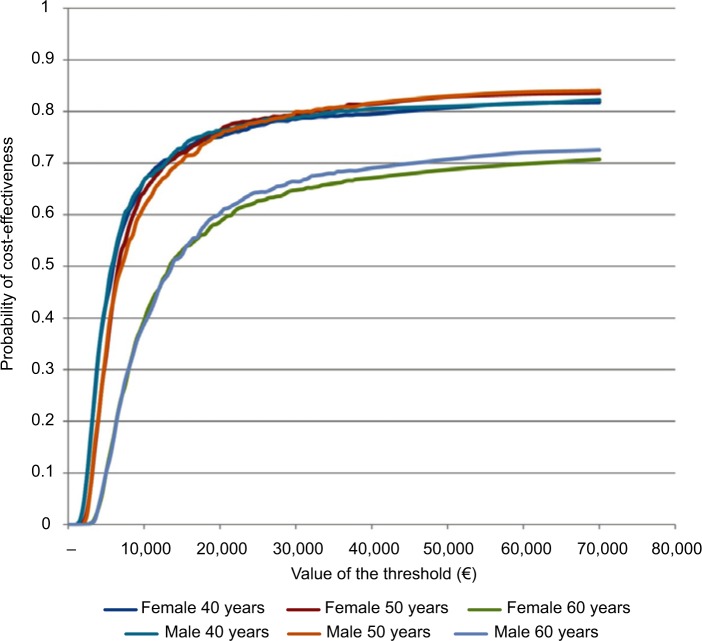
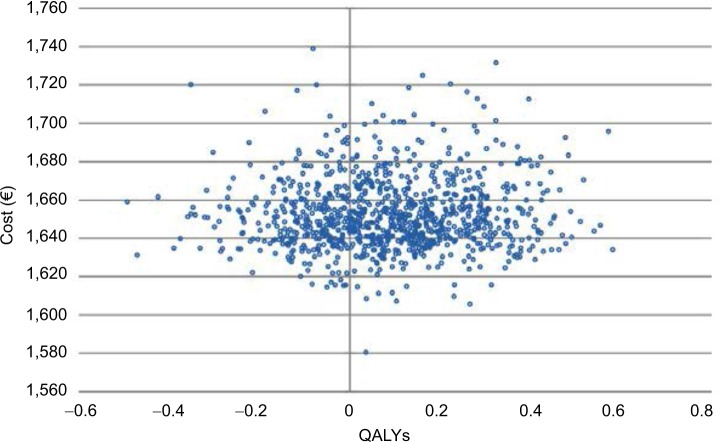
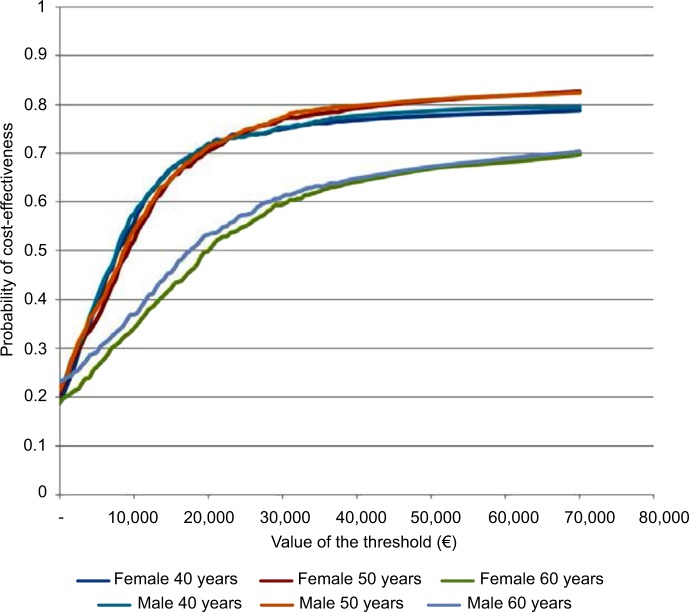
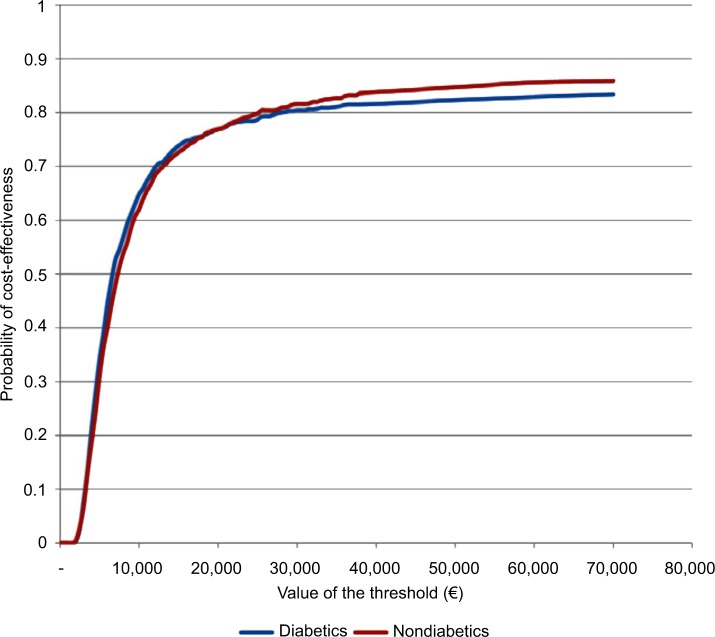
Methods: The analysis comprised a simulation based on the combined results of previous published studies, with the following steps: 1) estimation of the survival function of HF-HD patients from a clinical trial and of HDF patients using the risk reduction estimated in a meta-analysis; 2) simulation of the survival of the same sample of patients as if allocated to HF-HD or HDF using three-state Markov models; and 3) application of state-specific health-related quality of life coefficients and differential costs derived from the literature. Several Monte Carlo simulations were performed, including simulations for patients with different risk profiles, for example, by age (patients aged 40, 50, and 60 years), sex, and diabetic status. Scatter plots of simulations in the cost-effectiveness plane were produced, incremental cost-effectiveness ratios were estimated, and cost-effectiveness acceptability curves were computed.
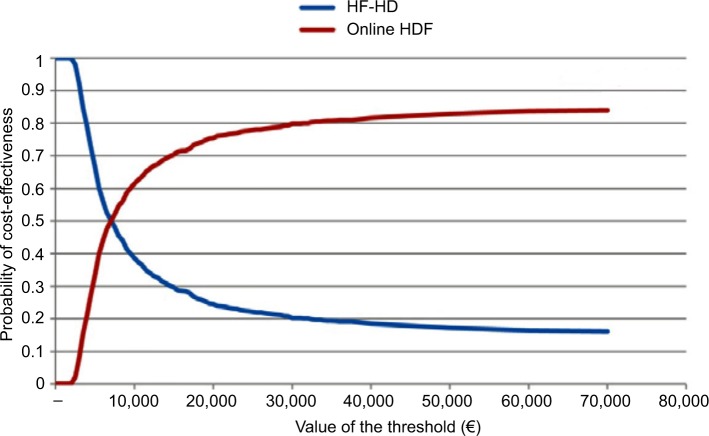
Results: An incremental cost-effectiveness ratio of €6,982/quality-adjusted life years (QALY) was estimated for the baseline cohort of 50-year-old male patients. Given the commonly accepted threshold of €40,000/QALY, HDF is cost-effective. The probabilistic sensitivity analysis showed that HDF is cost-effective with a probability of ~81% at a threshold of €40,000/QALY. It is fundamental to measure the outcome also in terms of quality of life. HDF is more cost-effective for younger patients.
Conclusion: HDF can be considered cost-effective compared to HF-HD.
Keywords: cost-effectiveness; hemodiafiltration; hemodialysis.
Figures
References
-
- Sichart JM, Moeller S. Utilization of hemodiafiltration as treatment modality in renal replacement therapy for end-stage renal disease patients – a global perspective. Contrib Nephrol. 2011;175:163–169. - PubMed
-
- Canaud B, Bragg-Gresham JL, Marshall MR, et al. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int. 2006;69(11):2087–2093. - PubMed
-
- Canaud B, Bayh I, Marcelli D, et al. Improved survival of incident patients with high-volume haemodiafiltration: a propensity-matched cohort study with inverse probability of censoring weighting. Nephron. 2015;129(3):179–188. - PubMed
-
- Akizawa T, Koiwa F. Clinical expectation of online hemodiafiltration: a Japanese perspective. Blood Purif. 2015;40(Suppl 1):12–16. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
