Justification for Rhinoseptoplasty in Children - Our 10 Years Overview
- PMID: 27703562
- PMCID: PMC5042622
- DOI: 10.3889/oamjms.2016.080
Justification for Rhinoseptoplasty in Children - Our 10 Years Overview
Abstract
Background: Nasal septal surgery and rhinoplasty are controversial in children. Traditionally, an attitude of restraint has been employed by most surgeons till an empirical age of 16 to 18 years. This is to avoid the possible adverse effects that the growth spurts may have on the nose and midface region.
Aim: The aim of this paper was to present the results of rhinoplasty in children in order to restore the anatomy and function or to promote normal development and outgrowth of the nose.
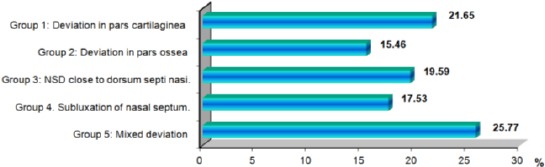
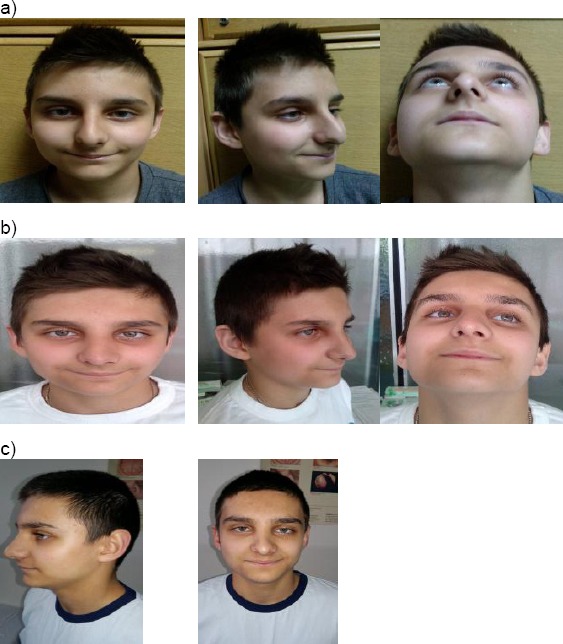
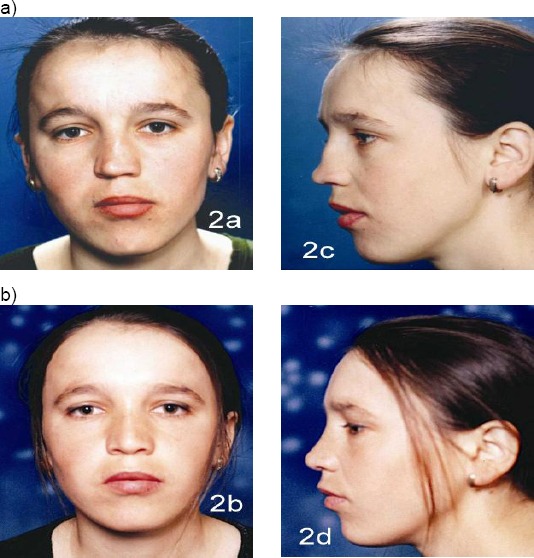
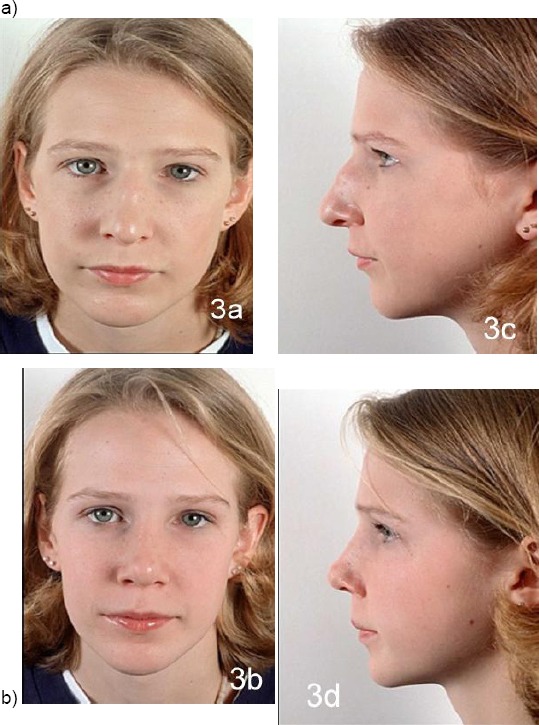
Material and methods: Ninety seven children aged 6-14, with severe nose deformities and breathing problems through the nose, were admitted for septo/rhinoplasty at the University Clinic for Ear, Nose and Throat, Faculty of Medicine, Ss Cyril and Methodius University of Skopje, Republic of Macedonia. At our Clinic, they have been observed and photographed (with parent permission) in the period of 10 years (2006-2016). The most frequent cause of these deformities was the nasal trauma in early childhood which was ignored or untreated. All of them rhino/septoplasty were indicated in accordance with the above-mentioned recommendations for rhino/septoplasty in early childhood and in adolescents.
Results: In 51 children and adolescents septoplasty were prepared. Mostly there was a group of younger children age from 6-10 (68%) and adolescents (32%). In the other 31 children and adolescents, septorhinoplasty was prepared. Mostly there were children older than 12 years old and adolescents (70%). Only 30% were younger than 12 years, of course with severe nasal breathing problems, nasal septal deformities and deformities of the nasal pyramid.
Conclusion: The growth centres of the nose have to be avoided if possible; long-term nasal issues will theoretically be minimised. If the surgeon replaces it, the cartilage of the nose becomes straighter but still intact.
Keywords: indications; midfacial development; nasal growth; septo/rhinoplasty in children; surgical procedures.
Figures




References
-
- Poublon RML, Verwoerd CDA, Verwoerd-Verhoef HL. Anatomy of the upper lateral cartilages in the human newborn. Rhinology. 1990;28:41–46. PMid:2336524. - PubMed
-
- Verwoerd CDA, van Loosen J, Schutte HE, Verwoerd-Verhoef HL, van Velzen D. Surgical aspects of the anatomy of the vomer in children and adults. Rhinology. 1989;9:87–96. - PubMed
-
- Potsic WP, Cotton RT, Handler SD, Zur KB, editors. Surgical Pediatric Otolaryngology. 2nd ed. Thieme: 2016. p. 900.
-
- NolstTrenite GJ, Verwoerd CDA, Verwoerd-Verhoef HL. Rhinology. Vol. 25. New York: Thieme medical publishers; 1987. Reimplantation of autologous septal cartilage in the growing nasal septum I. The influence of resection and reimplantation of septal cartilage upon nasal growth: an experimental study in growing rabbits; pp. 225–236. 1997; 168-180. - PubMed
-
- Graber TM. Orthodontics: Principles and Practice. Philadelphia: WB Saunders; 1966. Postnatal development of cranial, facial and oral structures: the dynamics of facial growth; pp. 69–78.
LinkOut - more resources
Full Text Sources
Other Literature Sources