

Long-term antipsychotic treatment in schizophrenia: systematic review and network meta-analysis of randomised controlled trials
- PMID: 27703755
- PMCID: PMC4995551
- DOI: 10.1192/bjpo.bp.115.002576
Long-term antipsychotic treatment in schizophrenia: systematic review and network meta-analysis of randomised controlled trials
Abstract
Background: For treatment of patients diagnosed with schizophrenia, comparative long-term effectiveness of antipsychotic drugs to reduce relapses when minimising adverse effects is of clinical interest, hence prompting this review.
Aims: To evaluate the comparative long-term effectiveness of antipsychotic drugs.
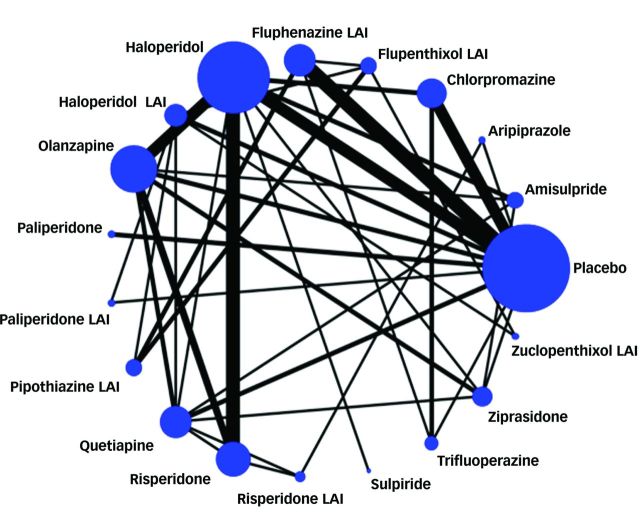
Method: We systematically searched electronic databases for reports of randomised controlled trials (RCTs) of antipsychotic monotherapy aimed at reducing relapse risks in schizophrenia. We conducted network meta-analysis of 18 antipsychotics and placebo.
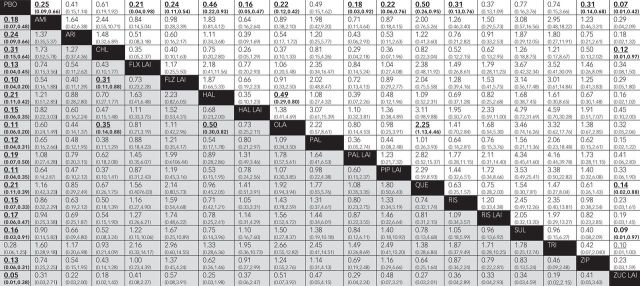
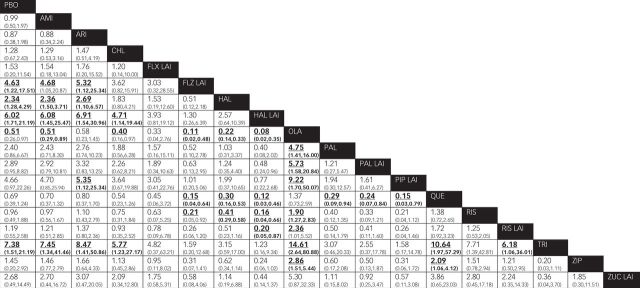
Results: Studies of 10 177 patients in 56 reports were included; treatment duration averaged 48 weeks (range 4-156). Olanzapine was significantly more effective than chlorpromazine (odds ratio (OR) 0.35, 95% CI 0.14-0.88) or haloperidol (OR=0.50, 95% CI 0.30-0.82); and fluphenazine decanoate was more effective than chlorpromazine (OR=0.31, 95% CI 0.11-0.88) in relapse reduction. Fluphenazine decanoate, haloperidol, haloperidol decanoate and trifluoperazine produced more extrapyramidal adverse effects than olanzapine or quetiapine; and olanzapine was associated with more weight gain than other agents.
Conclusions: Except for apparent superiority of olanzapine and fluphenazine decanoate over chlorpromazine, most agents showed intermediate efficacy for relapse prevention and differences among them were minor. Typical antipsychotics yielded adverse neurological effects, and olanzapine was associated with weight gain. The findings may contribute to evidence-based treatment selection for patients with chronic psychotic disorders.
Declaration of interest: R.J.B. received grants from the Bruce J. Anderson Foundation and the McLean Private Donors Psychopharmacology Research Fund.
Copyright and usage: © The Royal College of Psychiatrists 2016. This is an open access article distributed under the terms of the Creative Commons Non-Commercial, No Derivatives (CC BY-NC-ND) licence.
Figures


References
-
- Andreasen NC. Symptoms, signs, and diagnosis of schizophrenia. Lancet 1995; 346: 477–81. - PubMed
-
- Wyatt RJ. Neuroleptics and the natural course of schizophrenia. Schizophr Bull 1991; 17: 325–51. - PubMed
-
- Rettenbacher MA, Hofer A, Eder U, et al. Compliance in schizophrenia: psychopathology, side effects, and patients’ attitudes toward the illness and medication. J Clin Psychiatry 2004; 65: 1211–18. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
