

Advanced Hemodynamic Management in Patients with Septic Shock
- PMID: 27703980
- PMCID: PMC5039281
- DOI: 10.1155/2016/8268569
Advanced Hemodynamic Management in Patients with Septic Shock
Abstract
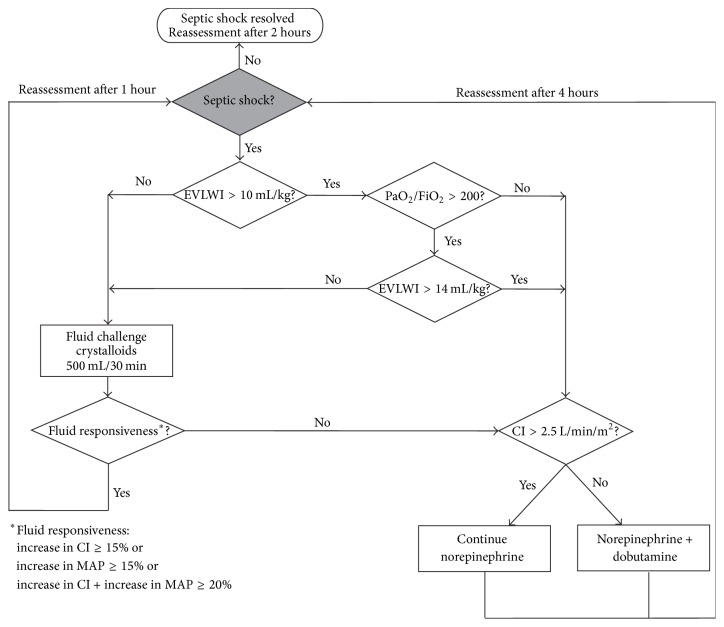
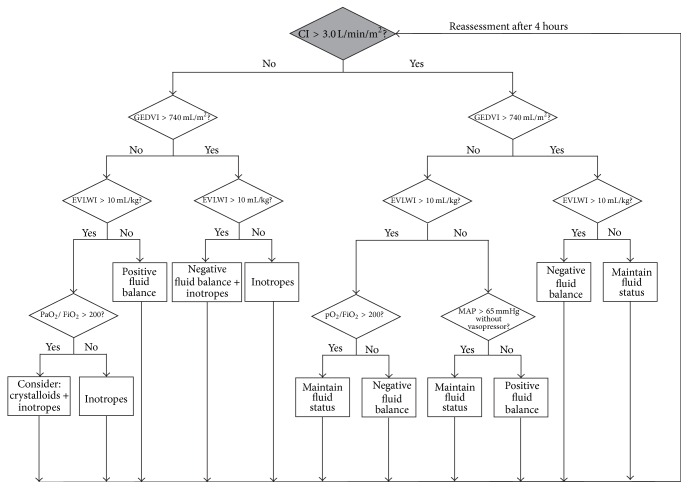
In patients with sepsis and septic shock, the hemodynamic management in both early and later phases of these "organ dysfunction syndromes" is a key therapeutic component. It needs, however, to be differentiated between "early goal-directed therapy" (EGDT) as proposed for the first 6 hours of emergency department treatment by Rivers et al. in 2001 and "hemodynamic management" using advanced hemodynamic monitoring in the intensive care unit (ICU). Recent large trials demonstrated that nowadays protocolized EGDT does not seem to be superior to "usual care" in terms of a reduction in mortality in emergency department patients with early identified septic shock who promptly receive antibiotic therapy and fluid resuscitation. "Hemodynamic management" comprises (a) making the diagnosis of septic shock as one differential diagnosis of circulatory shock, (b) assessing the hemodynamic status including the identification of therapeutic conflicts, and (c) guiding therapeutic interventions. We propose two algorithms for hemodynamic management using transpulmonary thermodilution-derived variables aiming to optimize the cardiocirculatory and pulmonary status in adult ICU patients with septic shock. The complexity and heterogeneity of patients with septic shock implies that individualized approaches for hemodynamic management are mandatory. Defining individual hemodynamic target values for patients with septic shock in different phases of the disease must be the focus of future studies.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
