

Achieving remission of proteinuria in childhood CKD
- PMID: 27704256
- PMCID: PMC5915370
- DOI: 10.1007/s00467-016-3495-1
Achieving remission of proteinuria in childhood CKD
Abstract
Background: A multidrug treatment strategy that targets urinary proteins with an angiotensin-converting enzyme (ACE) inhibitor and angiotensin receptor blocker (ARB) up-titrated to the respective maximum tolerated dose combined with intensified blood pressure (BP) control has been found to prevent renal function loss in adults with proteinuric nephropathies. Herein, we investigated the effects of this treatment protocol in the pediatric patient population.
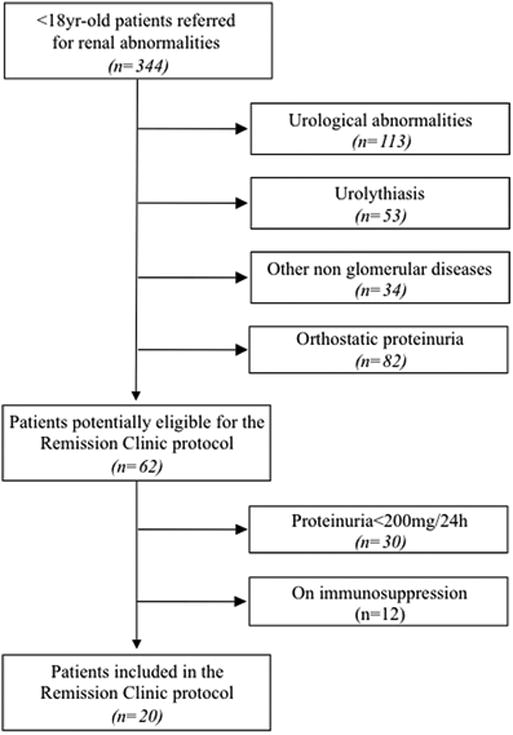
Methods: From May 2002 to September 2014 we included in this observational, longitudinal, cohort study 20 consecutive children with chronic nephropathies and 24-h proteinuria of >200 mg who had received ramipril and losartan up-titrated to the respective maximum approved and tolerated doses [mean (standard deviation) dose:2.48 (1.37) mg/m2 and 0.61 (0.46) mg/kg daily, respectively]. The primary efficacy endpoint was a >50 % reduction in 24-h proteinuria to <200 mg (remission). Secondary outcomes included changes in proteinuria, serum albumin, BP, and glomerular filtration rate (GFR).
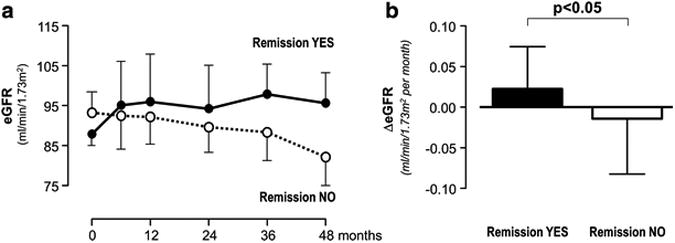
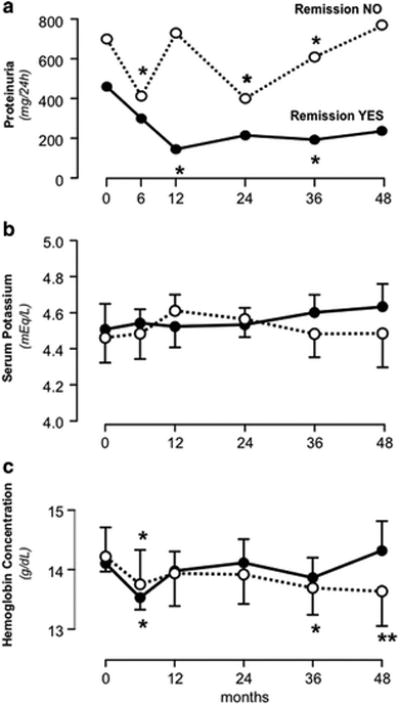
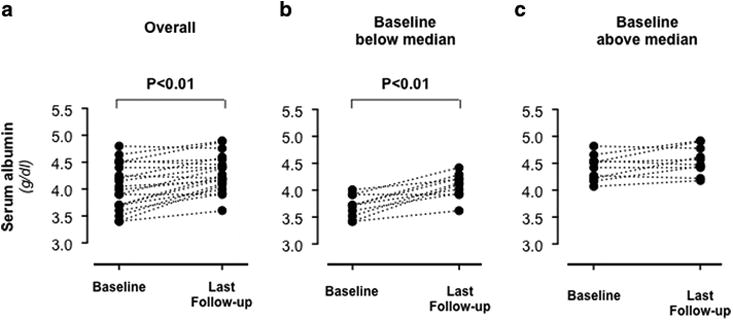
Results: Mean (± standard deviation) patient age at inclusion was 13.8 ± 2.8 years, and the median [interquartile range (IQR)] serum creatinine level and proteinuria were 0.7 (0.6-1.0) mg/dl and 690 (379-1270) mg/24 h or 435 (252-711) mg/m2/24 h, respectively. Proteinuria significantly decreased by month 6 of follow-up, and serum albumin levels increased over a median follow-up period of 78 (IQR 39-105) months. In the nine children who achieved remission, proteinuria reduction persisted throughout the whole follow-up without rebounds. The GFR improved in those children who achieved remission and worsened in those who did not. The mean GFR slopes differed significantly between these two groups (p < 0.05), being positive in those children with remission and negative in those without remission (+0.023 ± 0.15 vs.-0.014 ± 0.23 ml/min/1.73 m2/month, respectively), whereas BP control was similar between the two groups. Hyperkalemia was observed in two children.
Conclusions: Combination therapy with maximum approved doses of ACE inhibitors and ARBs is a safe strategy which may achieve proteinuria remission with kidney function stabilization or even improvement in a substantial proportion of children with proteinuric nephropathies.
Keywords: ACE inhibitor; Angiotensin receptor blocker; Children; Chronic nephropathy; Proteinuria.
Conflict of interest statement
Figures
References
-
- Ruggenenti P, Cravedi P, Remuzzi G. Mechanisms and treatment of CKD. J Am Soc Nephrol. 2012;23:1917–1928. - PubMed
-
- Ruggenenti P, Remuzzi G. Time to abandon microalbuminuria? Kidney Int. 2006;70:1214–1222. - PubMed
-
- Ruggenenti P, Perna A, Remuzzi G, Investigators GG. Retarding progression of chronic renal disease: the neglected issue of residual proteinuria. Kidney Int. 2003;63:2254–2261. - PubMed
-
- Arbus GS, Poucell S, Bacheyie GS, Baumal R. Focal segmental glomerulosclerosis with idiopathic nephrotic syndrome: three types of clinical response. J Pediatr. 1982;101:40–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
