

Foreign Bodies in the Urinary Bladder and Their Management: A Single-Centre Experience From North India
- PMID: 27706010
- PMCID: PMC5083828
- DOI: 10.5213/inj.1632524.262
Foreign Bodies in the Urinary Bladder and Their Management: A Single-Centre Experience From North India
Abstract
Purpose: This study was performed to characterise the nature, clinical presentation, mode of insertion, and management of intravesical foreign bodies in patients treated at our hospital.
Methods: Between January 2008 and December 2014, 49 patients were treated for intravesical foreign bodies at King George Medical University, Lucknow. All records of these patients were retrospectively analysed to characterise the nature of the foreign body, each patient's clinical presentation, the mode of insertion, and how the case was managed.
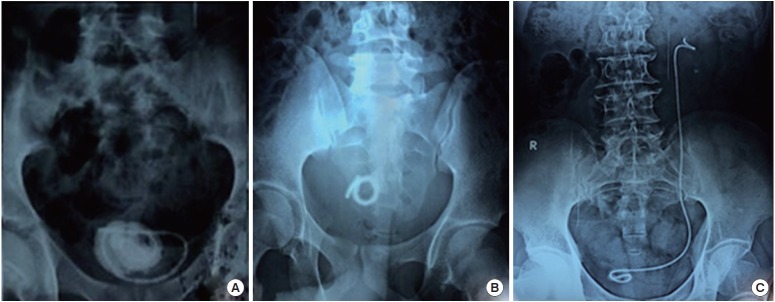
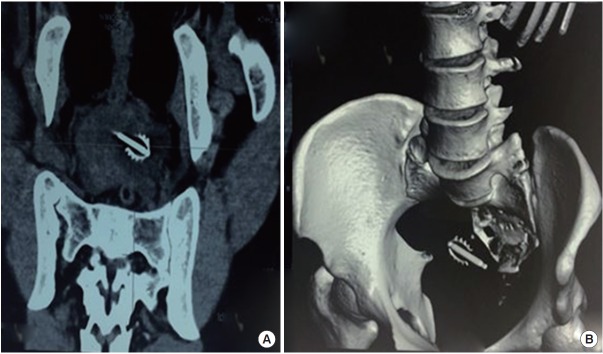
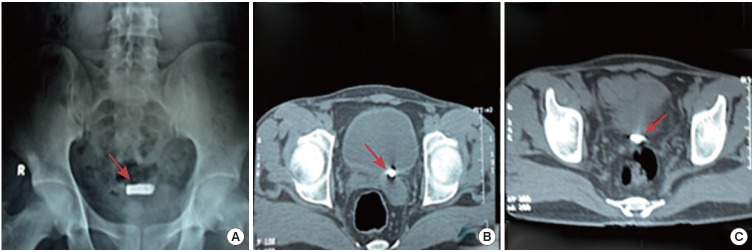
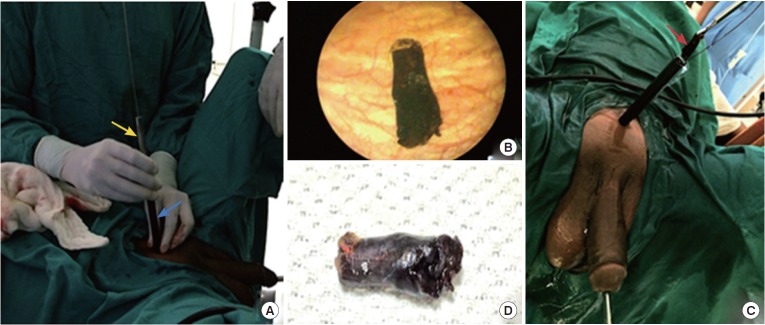
Results: A total of 49 foreign bodies were retrieved from patients' urinary bladders during the study period. The patients ranged in age from 11 to 68 years. Thirty-three patients presented with complaints of haematuria (67.3%), 29 complained of frequency of urination and dysuria (59.1%), and 5 patients reported pelvic pain (10.2%). The circumstances of insertion were iatrogenic in 20 cases (40.8%), self-insertion in 17 cases (34.6%), sexual abuse in 4 cases (8.1%), migration from another organ in 4 cases (8.1%), and assault in 4 cases (8.1%). Of the foreign bodies, 33 (67.3%) were retrieved by cystoscopy, while transurethral cystolitholapaxy was required in 10 patients (20.4%), percutaneous suprapubic cystolitholapaxy was performed in 4 patients (8.1%), and holmium laser lithotripsy was performed in 2 patients (4.08%).
Conclusions: Foreign bodies should always be included in the differential diagnosis when evaluating a patient who presents with chronic lower urinary tract symptoms. A large percentage of foreign bodies can be retrieved using endoscopic techniques. Open surgical removal may be performed in cases where endoscopic techniques are unsuitable or have failed.
Keywords: Endoscopy; Foreign Bodies; Iatrogenic Disease; Urinary Bladder.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Foreign bodies in the urinary bladder and their management: a Pakistani experience.Singapore Med J. 2011 Jan;52(1):24-8. Singapore Med J. 2011. PMID: 21298237
-
Intravesical foreign bodies: review and current management strategies.Urol J. 2008 Fall;5(4):223-31. Urol J. 2008. PMID: 19101894
-
Management of intravesical self-inflicted sharp objects in children: 10-year single-center experience.J Pediatr Urol. 2016 Apr;12(2):97.e1-5. doi: 10.1016/j.jpurol.2015.06.020. Epub 2015 Sep 18. J Pediatr Urol. 2016. PMID: 26468014
-
[Voiding symptoms as presentation of an intravesical foreign body].Arch Esp Urol. 2008 Sep;61(7):781-5. Arch Esp Urol. 2008. PMID: 18972912 Review. Spanish.
-
Evaluation of holmium laser for managing mesh/suture complications of continence surgery.BJU Int. 2011 Nov;108(9):1472-8. doi: 10.1111/j.1464-410X.2010.10012.x. Epub 2011 Jan 13. BJU Int. 2011. PMID: 21231987 Review.
Cited by
-
Small spherical foreign bodies in the genitourinary tract and their management.BMC Pediatr. 2022 Jan 15;22(1):42. doi: 10.1186/s12887-022-03114-7. BMC Pediatr. 2022. PMID: 35033033 Free PMC article.
-
Foreign Body in the Male Urinary Bladder: A Case Report.Cureus. 2024 Feb 21;16(2):e54592. doi: 10.7759/cureus.54592. eCollection 2024 Feb. Cureus. 2024. PMID: 38523921 Free PMC article.
-
Foreign bodies in children's lower urinary tract: A case series and literature review.Front Pediatr. 2023 Jan 10;10:1095993. doi: 10.3389/fped.2022.1095993. eCollection 2022. Front Pediatr. 2023. PMID: 36704132 Free PMC article.
-
An earphone wire inside the urinary bladder: A case report and comprehensive literature review of genitourinary polyembolokoilamania.Radiol Case Rep. 2022 Mar 2;17(5):1457-1463. doi: 10.1016/j.radcr.2022.01.080. eCollection 2022 May. Radiol Case Rep. 2022. PMID: 35265240 Free PMC article.
-
A childhood blast victim presenting with bladder stone in adulthood-A rare case report of retained blast fragment with secondary stone.Urol Case Rep. 2022 Mar 25;43:102066. doi: 10.1016/j.eucr.2022.102066. eCollection 2022 Jul. Urol Case Rep. 2022. PMID: 35444927 Free PMC article.
References
-
- Sukkarieh T, Smaldone M, Shah B. Multiple foreign bodies in the anterior and posterior urethra. Int Braz J Urol. 2004;30:219–20. - PubMed
-
- Ejstrud P, Poulsen J. Laparoscopic removal of an electric wire from the bladder. Br J Urol. 1997;80:338. - PubMed
-
- Andrews NJ, Hall CN, Taylor TV. Colovesical fistula caused by a chicken bone. Br J Urol. 1988;62:617. - PubMed
-
- Potter D, Smith D, Shorthouse AJ. Colovesical fistula following ingestion of a foreign body. Br J Urol. 1998;81:499–500. - PubMed
-
- Nishiyama K, Shimada T, Yagi S, Kawahara M, Nakagawa M. Endoscopic removal of intravesical thermometer using a rigid nephroscope and forceps. Int J Urol. 2002;9:717–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
