

Incidences and Risk Factors of Organ Manifestations in the Early Course of Systemic Sclerosis: A Longitudinal EUSTAR Study
- PMID: 27706206
- PMCID: PMC5051961
- DOI: 10.1371/journal.pone.0163894
Incidences and Risk Factors of Organ Manifestations in the Early Course of Systemic Sclerosis: A Longitudinal EUSTAR Study
Abstract
Objective: Systemic sclerosis (SSc) is a rare and clinically heterogeneous autoimmune disorder characterised by fibrosis and microvascular obliteration of the skin and internal organs. Organ involvement mostly manifests after a variable period of the onset of Raynaud's phenomenon (RP). We aimed to map the incidence and predictors of pulmonary, cardiac, gastrointestinal (GI) and renal involvement in the early course of SSc.
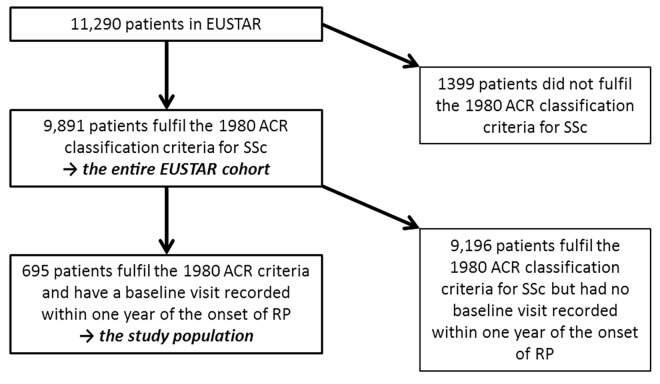
Methods: In the EUSTAR cohort, patients with early SSc were identified as those who had a visit within the first year after RP onset. Incident SSc organ manifestations and their risk factors were assessed using Kaplan-Meier methods and Cox regression analysis.
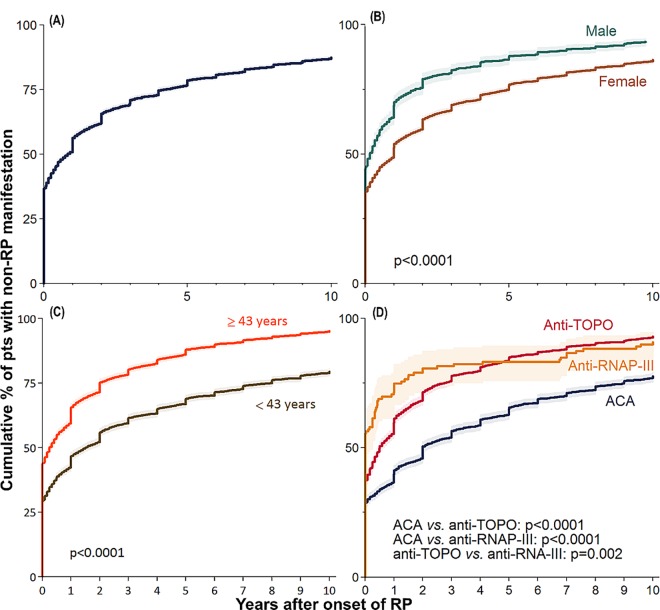
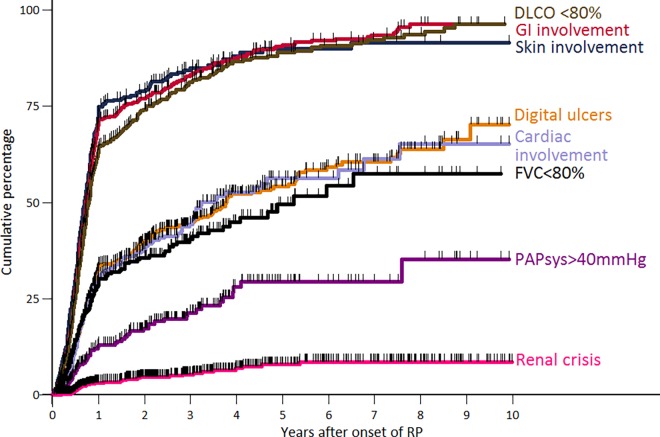
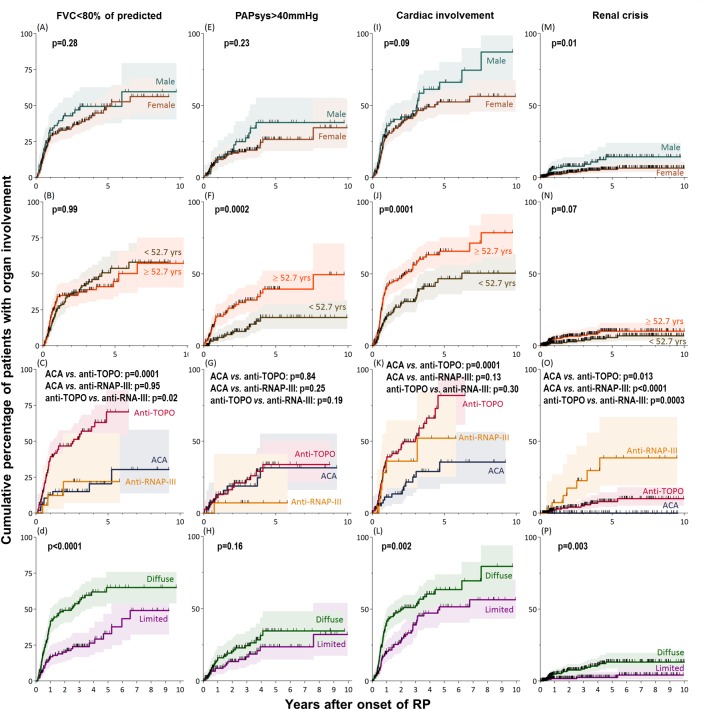
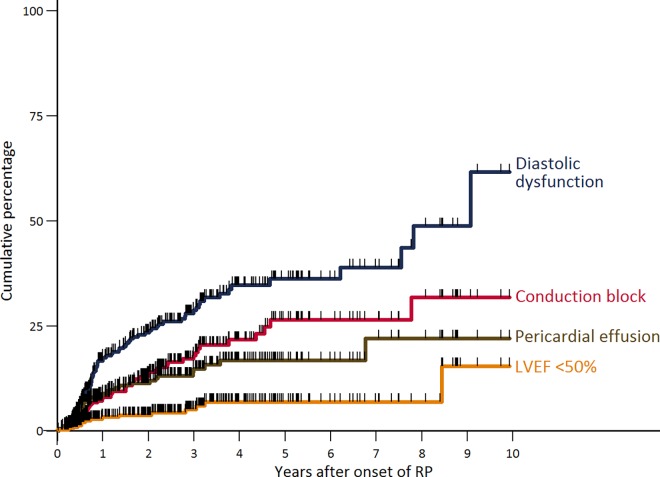
Results: Of the 695 SSc patients who had a baseline visit within 1 year after RP onset, the incident non-RP manifestations (in order of frequency) were: skin sclerosis (75%) GI symptoms (71%), impaired diffusing capacity for monoxide<80% predicted (65%), DU (34%), cardiac involvement (32%), FVC<80% predicted (31%), increased PAPsys>40mmHg (14%), and renal crisis (3%). In the heart, incidence rates were highest for diastolic dysfunction, followed by conduction blocks and pericardial effusion. While the main baseline risk factor for a short timespan to develop FVC impairment was diffuse skin involvement, for PAPsys>40mmHg it was higher patient age. The main risk factors for incident cardiac manifestations were anti-topoisomerase autoantibody positivity and older age. Male sex, anti-RNA-polymerase-III positivity, and older age were risk factors associated with incident renal crisis.
Conclusion: In SSc patients presenting early after RP onset, approximately half of all incident organ manifestations occur within 2 years and have a simultaneous rather than a sequential onset. These findings have implications for the design of new diagnostic and therapeutic strategies aimed to 'widen' the still very narrow 'window of opportunity'. They may also enable physicians to counsel and manage patients presenting early in the course of SSc more accurately.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
