

Short- and long-term effects of oral vancomycin on the human intestinal microbiota
- PMID: 27707993
- PMCID: PMC5161046
- DOI: 10.1093/jac/dkw383
Short- and long-term effects of oral vancomycin on the human intestinal microbiota
Abstract
Background: Oral vancomycin remains the mainstay of therapy for severe infections produced by Clostridium difficile, the most prevalent cause of healthcare-associated infectious diarrhoea in developed countries. However, its short- and long-term effects on the human intestinal microbiota remain largely unknown.
Methods: We utilized high-throughput sequencing to analyse the effects of vancomycin on the faecal human microbiota up to 22 weeks post-antibiotic cessation. The clinical relevance of the observed microbiota perturbations was studied in mice.
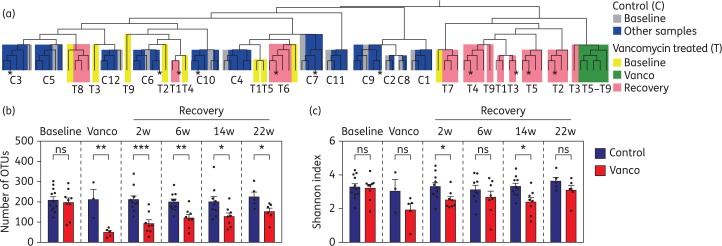
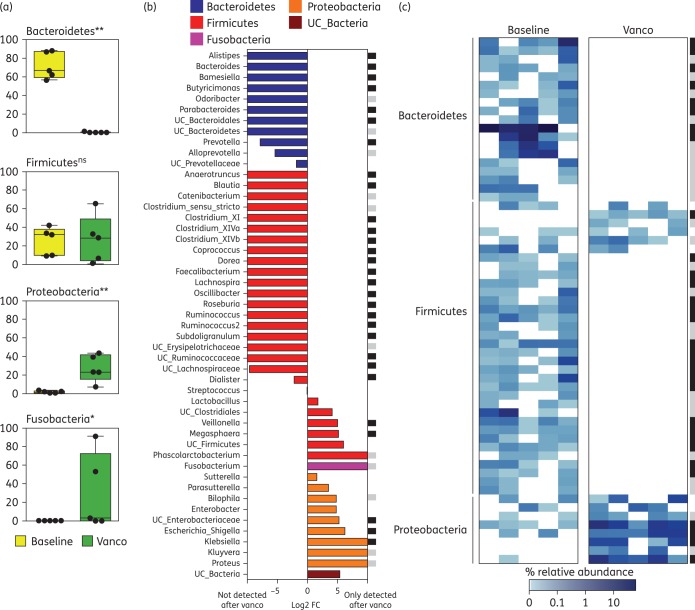
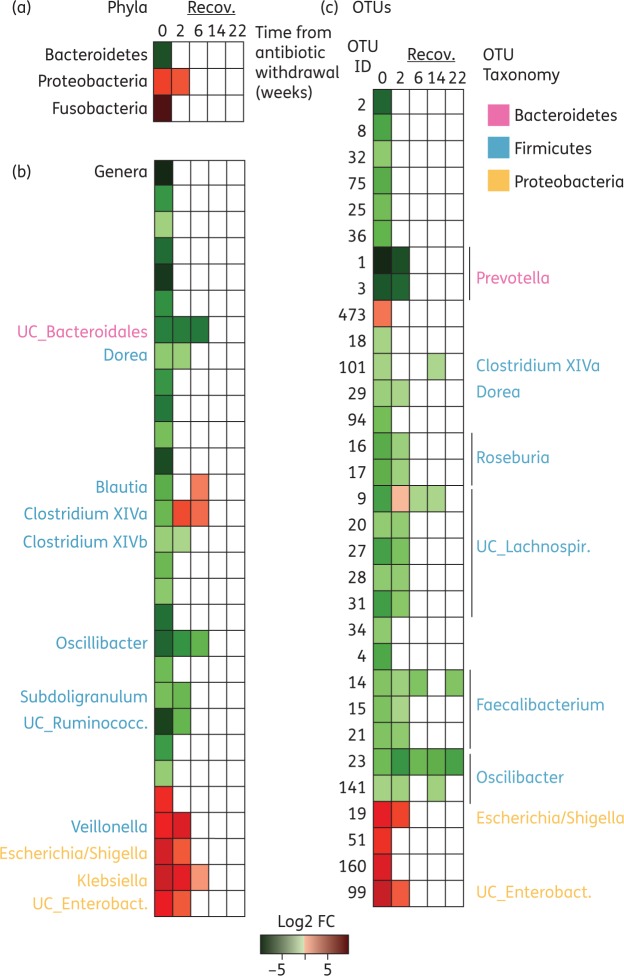
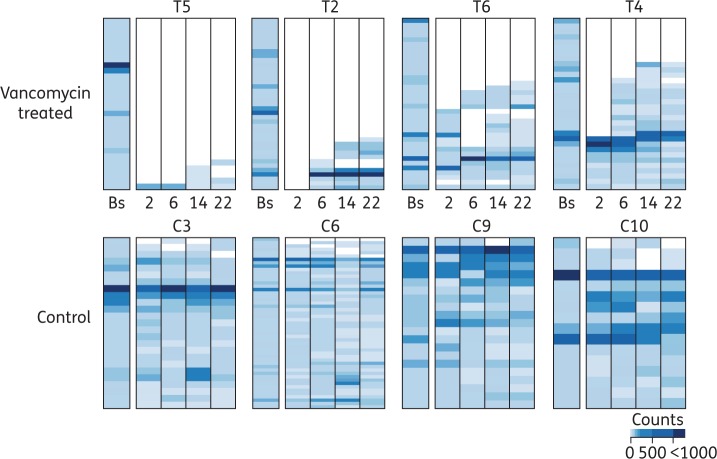
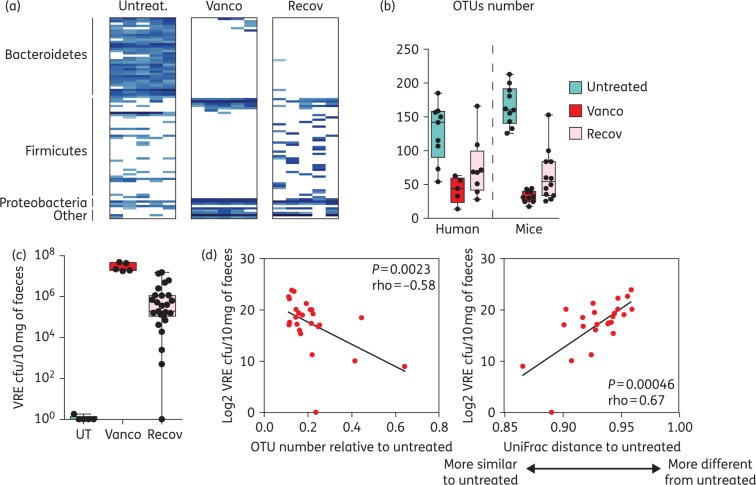
Results: During vancomycin therapy, most intestinal microbiota genera and operational taxonomic units (OTUs) were depleted in all analysed subjects, including all baseline OTUs from the phylum Bacteroidetes. This was accompanied by a vast expansion of genera associated with infections, including Klebsiella and Escherichia/Shigella. Following antibiotic cessation, marked differences in microbiota resilience were observed among subjects. While some individuals recovered a microbiota close to baseline composition, in others, up to 89% of abundant OTUs could no longer be detected. The clinical relevance of the observed microbiota changes was further demonstrated in mice, which developed analogous microbiota alterations. During vancomycin treatment, mice were highly susceptible to intestinal colonization by an antibiotic-resistant pathogen and, upon antibiotic cessation, a less-resilient microbiota allowed higher levels of pathogen colonization.
Conclusions: Oral vancomycin induces drastic and consistent changes in the human intestinal microbiota. Upon vancomycin cessation, the microbiota recovery rate varied considerably among subjects, which could influence, as validated in mice, the level of susceptibility to pathogen intestinal colonization. Our results demonstrate the negative long-term effects of vancomycin, which should be considered as a fundamental aspect of the cost-benefit equation for antibiotic prescription.
© The Author 2016. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures
References
-
- Rakoff-Nahoum S, Paglino J, Eslami-Varzaneh F et al. Recognition of commensal microflora by toll-like receptors is required for intestinal homeostasis. Cell 2004; 118: 229–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
