

Differential effects of peptidoglycan on colorectal tumors and intestinal tissue post-pelvic radiotherapy
- PMID: 27708223
- PMCID: PMC5342770
- DOI: 10.18632/oncotarget.12353
Differential effects of peptidoglycan on colorectal tumors and intestinal tissue post-pelvic radiotherapy
Abstract
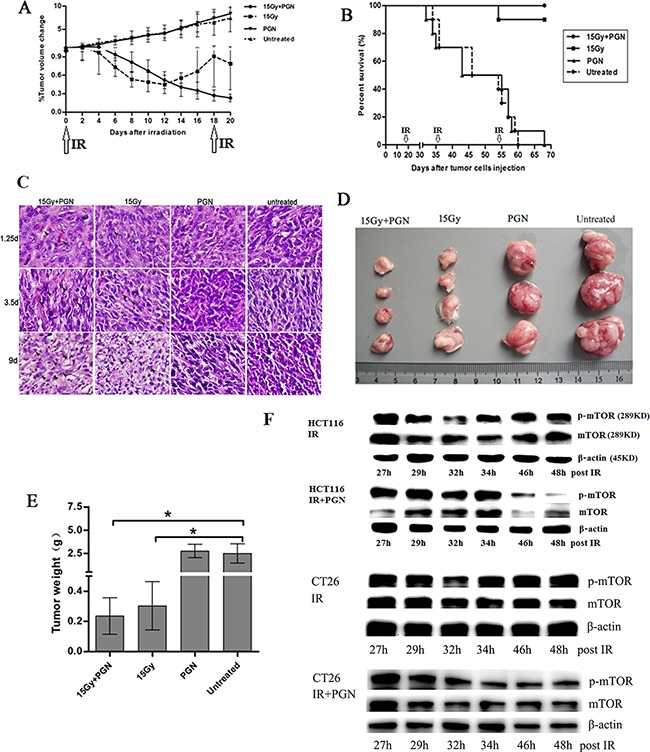
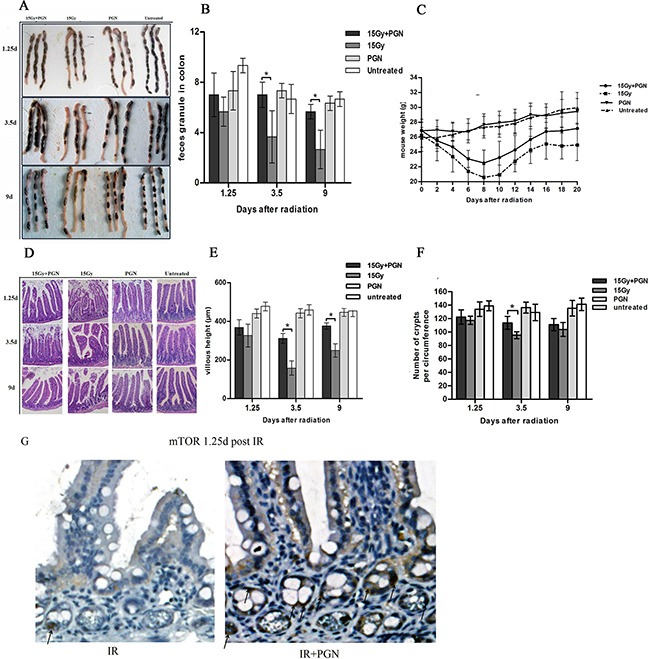
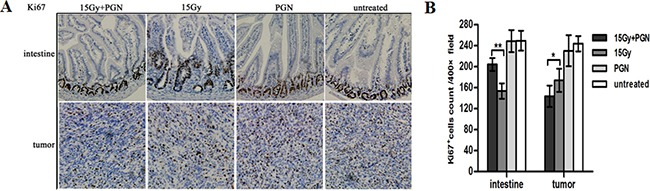
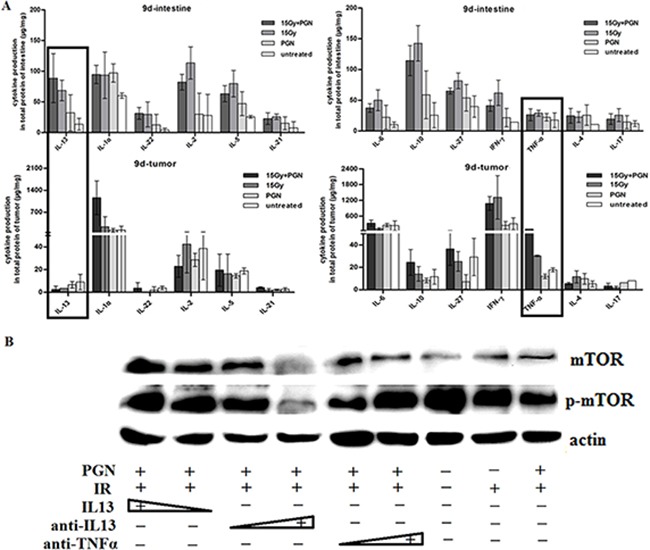
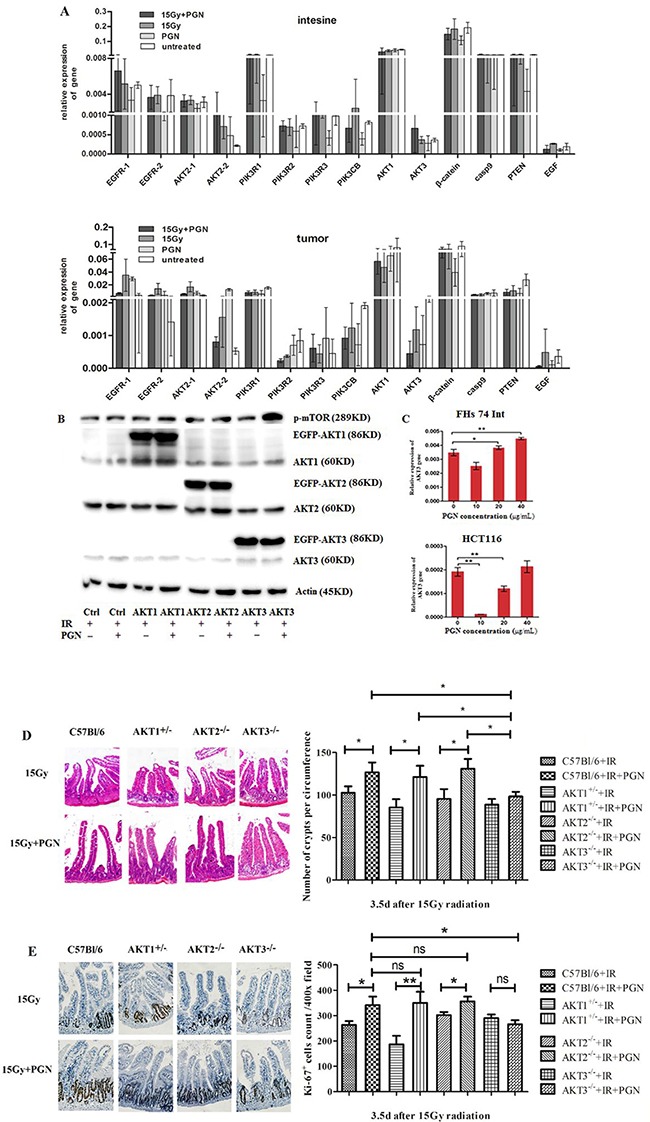
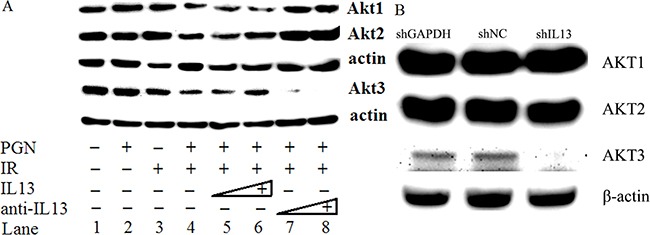
Immediate medical intervention is required after pelvic tumor radiotherapy to protect the radiosensitive intestine and also to mitigate tumor growth. Toll-like receptors (TLRs) have been shown to promote tissue repair processes. Here, we analyzed the effect observed upon combining the TLR2 agonist, peptidoglycan (PGN), with radiation therapy on tumors as well as intestinal tissue, both in vitro and in vivo. In contrast to radiotherapy alone, PGN when combined with ionizing radiation (IR) elicited enhanced antitumor effects and also reduced the IR-induced intestinal damage. Mechanistic studies showed that PGN first induced an IL13 response in the irradiated intestine, but was decreased in tumor cell models screened by Th1/Th2 FlowCytomix assay and validated by the application of IL13 and anti-IL13 neutralizing antibodies. Next, PGN stimulated Akt3, but not Akt1/2, as was verified by AKT1/2/3 plasmid transfection assay and in AKT1/2/3 knockout mice in vivo. Akt3 expression was inhibited in 20 μg/mL PGN-treated tumor cells and in 1.5 mg/kg PGN-treated mouse tumor models. However, Akt3 was raised via IL13 in the irradiated intestine and human intestinal cell line after the same treatment. Finally, PGN activated mTOR via IL13/AKT3 in the intestine and restored intestinal structure and function. As an adjuvant to radiotherapy, PGN inhibited tumorigenesis by suppression of mTOR activity. To summarize, the IL13/AKT3/mTOR pathway was lessened in PGN-treated irradiated tumors but was raised in the normal intestine tissue. This distinct effect of PGN on normal and tumor tissues during pelvic radiotherapy suggests that PGN may be a promising adjuvant therapy to radiation.
Keywords: IL13-AKT3-mTOR pathway; colorectal tumor; intestine; pelvic radiotherapy; peptidoglycan.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Andreyev HJN. Gastrointestinal Problems after Pelvic Radiotherapy: the Past, the Present and the Future. Clinical Oncology. 2007;19:790–799. - PubMed
-
- Andreyev J. Gastrointestinal symptoms after pelvic radiotherapy: a new understanding to improve management of symptomatic patients. Lancet Oncol. 2007;8:1007–1017. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
