

Neurohormonal activation in heart failure with reduced ejection fraction
- PMID: 27708278
- PMCID: PMC5286912
- DOI: 10.1038/nrcardio.2016.163
Neurohormonal activation in heart failure with reduced ejection fraction
Abstract
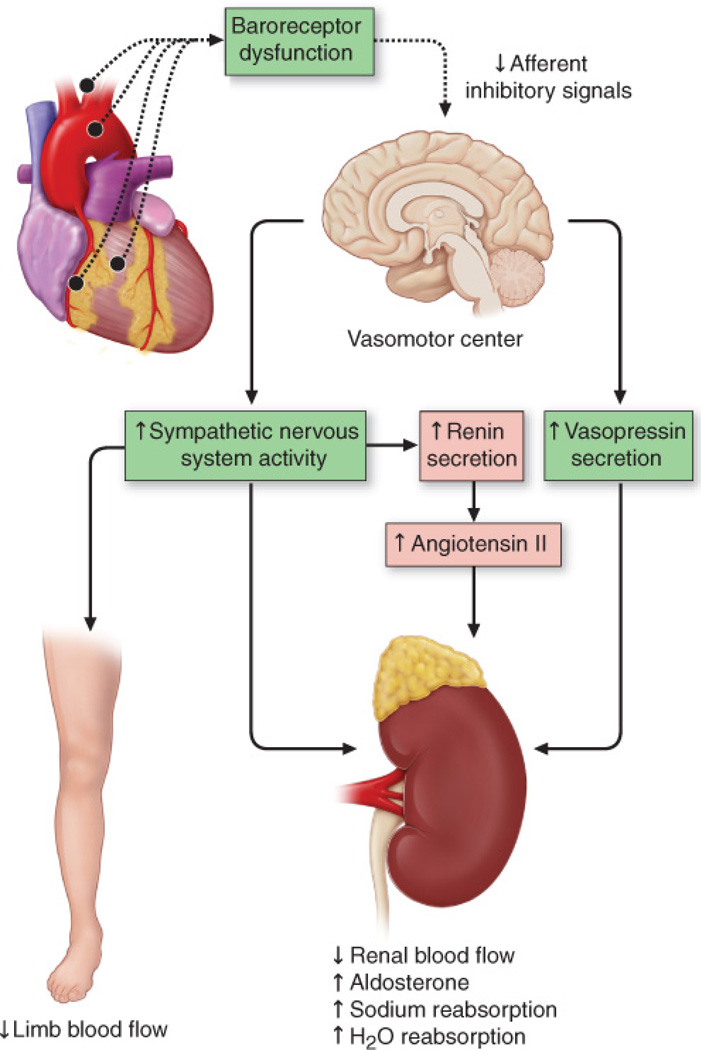
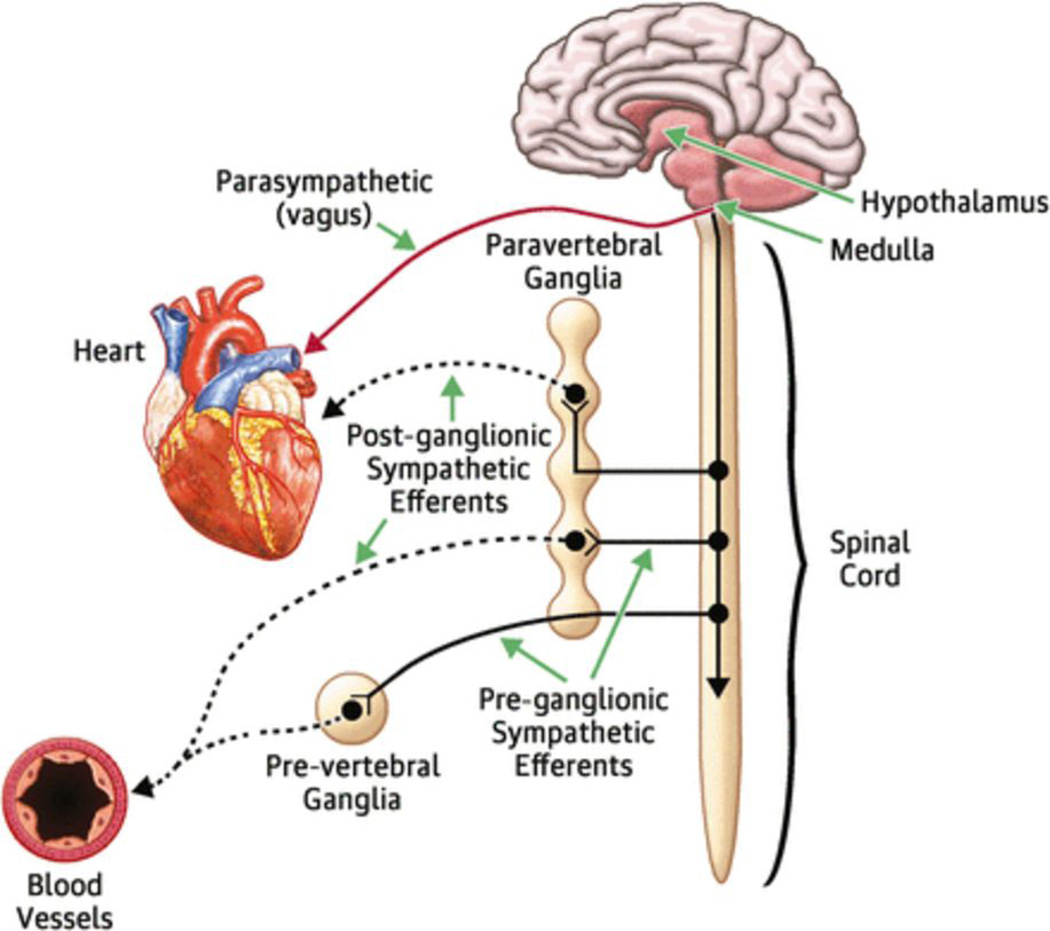
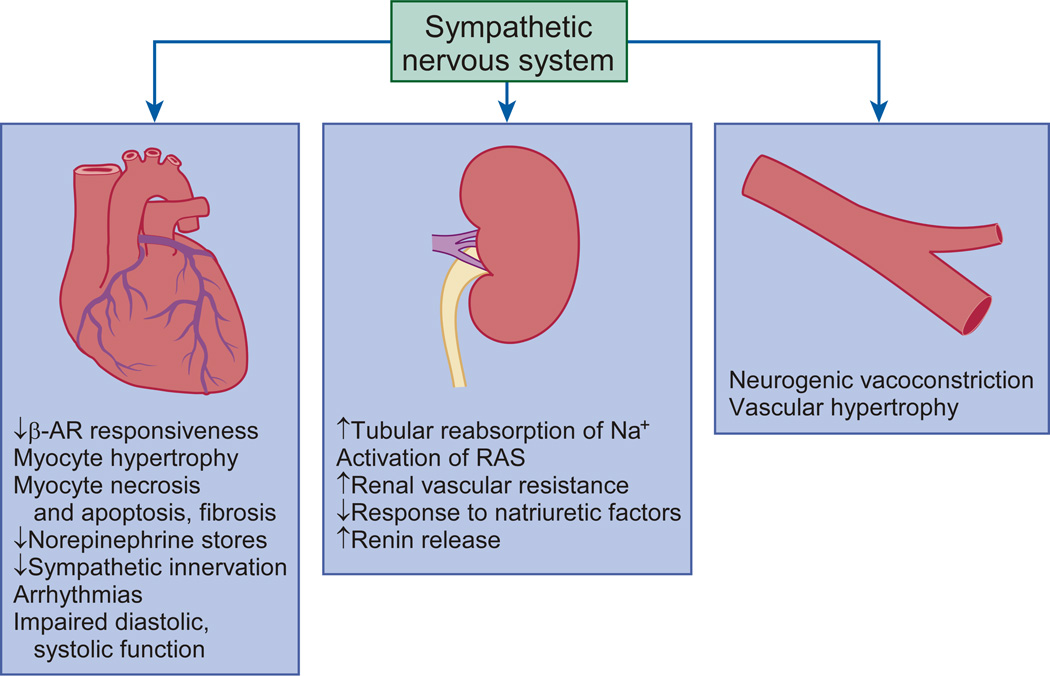
Heart failure with reduced ejection fraction (HFrEF) develops when cardiac output falls as a result of cardiac injury. The most well-recognized of the compensatory homeostatic responses to a fall in cardiac output are activation of the sympathetic nervous system and the renin-angiotensin-aldosterone system (RAAS). In the short term, these 'neurohormonal' systems induce a number of changes in the heart, kidneys, and vasculature that are designed to maintain cardiovascular homeostasis. However, with chronic activation, these responses result in haemodynamic stress and exert deleterious effects on the heart and the circulation. Neurohormonal activation is now known to be one of the most important mechanisms underlying the progression of heart failure, and therapeutic antagonism of neurohormonal systems has become the cornerstone of contemporary pharmacotherapy for heart failure. In this Review, we discuss the effects of neurohormonal activation in HFrEF and highlight the mechanisms by which these systems contribute to disease progression.
Figures

References
-
- Rouleau JL, et al. Activation of neurohumoral systems following acute myocardial infarction. Am. J. Cardiol. 1991;68:80D–86D. - PubMed
-
- Packer M. The Neurohormonal Hypothesis: a theory to explain the mechanism of disease progression in heart failure. J. Am. Coll. Cardiol. 1992;20:248–254. - PubMed
-
- Piepoli M, et al. Contribution of muscle afferents to the hemodynamic, autonomic, and ventilatory responses to exercise in patients with chronic heart failure: effects of physical training. Circulation. 1996;93:940–952. - PubMed
-
- Giannoni A, et al. Combined increased chemosensitivity to hypoxia and hypercapnia as a prognosticator in heart failure. J Am Coll Cardiol. 2009;53:1975–1980. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
